Pathology Cases for Week 7
Pathology Case Descriptions
CASE NUMBER 92
[Aperio ImageScope] [Aperio WebScope]
Clinical History: A 65-year-old male complained about increasing dyspnea over the last 10 years. The dyspnea had suddenly increased and the patient was admitted with signs of heart failure. He died one week after admission from an acute brain infarct.
Image Gallery:
(Summary of Gross Findings - click here)
The lungs were very large and upon palpation there was marked crepitation.
|
(Summary of Microscopic Findings - click here)
The alveolar spaces are distended and the alveolar septa are thickened by fibrous tissue. Numerous "free floating" alveolar septa are present, recognizable as pieces at alveolar wall not connected at either end to adjacent septa.
|
(Review Normal Histology - click here)
Norm No. 24 Lung
[ImageScope] [WebScope]
The primary function of the lung is gas exchange. Therefore, alveoli have thin walls lined by thin flat pneumocytes and endothelial cells. There is no thickening or fibrosis of the interstitium. The bronchioli are lined with basally oriented ciliated columnar epithelium. The bronchi are lined by similar epithelium. There are mucous glands within the submucosa. The bronchial smooth muscle is not hypertrophied. The pulmonary vessels are patent with no evidence of intimal thickening or muscular hyperplasia.
|
92-1. What is the most likely diagnosis?
- Lung abscesses
- Panacinar emphysema
- Asbestosis
- Centrilobular emphysema
ANSWER
92-2. What factor contributed most to this patient’s disease?
- Living in South Carolina
- Genetics
- Cigarette smoking
- Alcohol consumption
ANSWER
CASE NUMBER 223
[Aperio ImageScope] [Aperio WebScope]
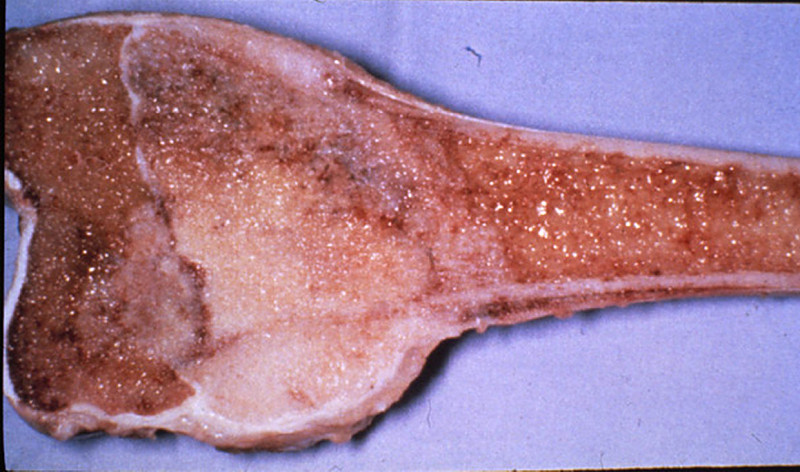
Clinical History: A 13-year-old male had an enlarging mass in the left thigh for 1 1/2 months. It was not associated with pain or tenderness. The X-ray revealed a large tumor extending around the entire shaft and lower 1/3 or the left femur. Amputation was performed after biopsy. Limb salvage surgery is commonly performed today.
Image Gallery:
(Summary of Gross Findings - click here)
The tumor was a large, pink-gray, soft and granular mass, 8x4x5 cm in size, involving the lower femoral shaft, and growing into the muscle.
|
(Summary of Microscopic Findings - click here)
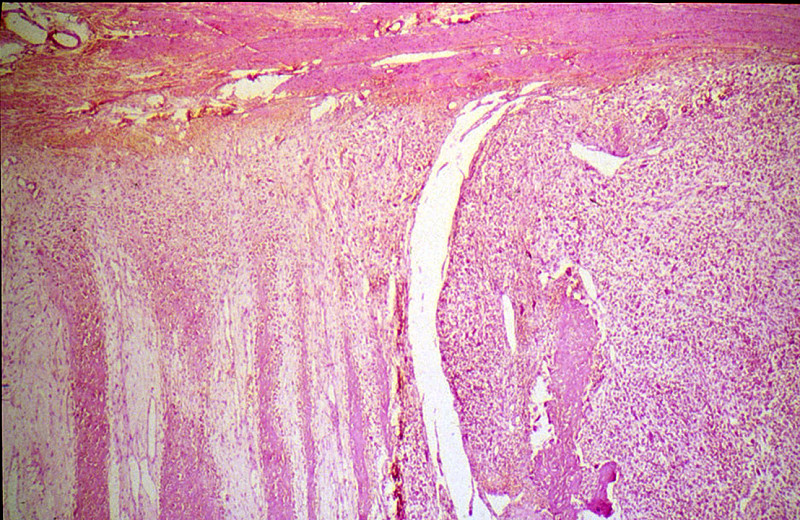
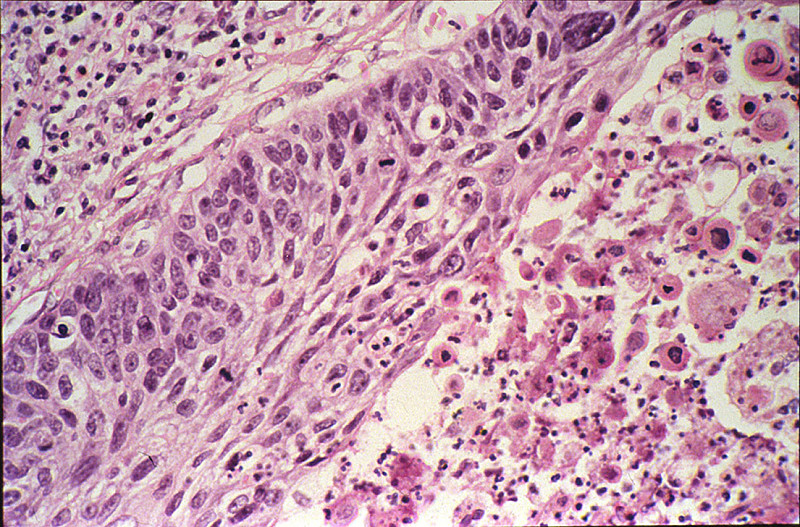
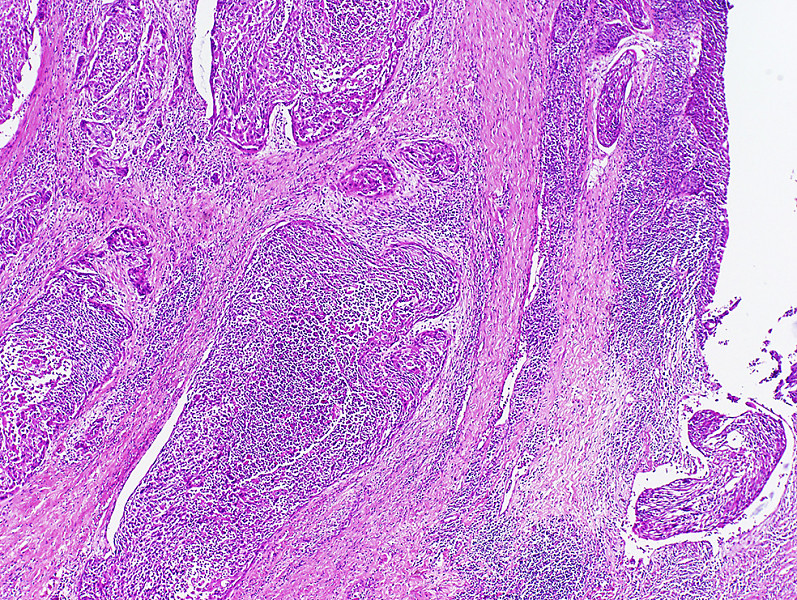
The tumor is composed of sheaths of loosely packed fibroblastic and osteoblastic cells, which have large hyperchromatic nuclei and scanty eosinophilic cytoplasm. In the intercellular spaces of the tumor there is deposition of pink homogeneous osteoid tissue which frequently transforms into irregular, bony trabeculae. New periosteal bone formation may be seen in the section.
|
(Review Normal Histology - click here)
Norm No. 10 Pubic symphysis
[ImageScope] [WebScope]
The pubic symphysis includes cartilage, bone, dense connective tissue and bone as well as skeletal muscles inserting into the bone.
|
223-1. This tumor comprises atypical osteoblastic cells that have large hyperchromatic nuclei with nuclear pleomorphism and frequent mitoses, producing new bone matrix (osteoid). The best diagnosis is:
- Osteoid osteoma
- Giant cell tumor of bone
- Osteosarcoma
- Ossifying fibroma
- Ewing’s sarcoma
ANSWER
223-2. Mutation and loss of function of the Rb and p53 genes are often encountered in this tumor. Both Rb and p53 are examples of:
- Oncogenes
- Tumor suppressor genes
- Mismatch repair genes
- Cyclin dependent kinase inhibitors
- Matrix metalloproteinases
ANSWER
CASE NUMBER 129
[Aperio ImageScope] [Aperio WebScope]
Clinical History: A 70-year-old white male had an insidious onset of dysphagia of six months duration. X-ray revealed a filling defect and stenosis in the lower esophagus. An esophageal resection was performed.
Image Gallery:
(Summary of Gross Findings - click here)
The resected esophagus contained a firm, raised, pink-gray, friable and necrotic 3.5 x 4.5 cm tumor mass, completely encircling the esophagus and producing a marked stenosis.
|
(Summary of Microscopic Findings - click here)
At one end of the section the squamous epithelium of the esophagus shows marked atypia, pleomorphism and loss of polarity, but no submucosal invasion. These changes represent carcinoma in situ. By following the mucosal lining, one comes upon an area where the cords and nests of poorly differentiated squamous cells are seen to invade the mucosa and submucosa reaching the muscular layer. At one margin of the section the tumor cells are better differentiated with production of keratin and formation of so-called epithelial pearls. Associated with the tumor are marked fibrous proliferation and intense chronic inflammatory infiltration in the stroma. The tumor invades into, but not through the muscularis externa.
|
(Review Normal Histology - click here)
Slide UCSF 226 (esophagus, H&E) WebScope ImageScope
Slide UMich 126 40x (trachea & esophagus, H&E) WebScope ImageScope
Slide UMich 153 20x (esophagus, H&E) WebScope ImageScope
Slide UMich 155 40x (gastro-esophageal junct, H&E) WebScope ImageScope
For the purpose of histological descriptions, the esophagus is subdivided into upper (entirely skeletal muscle in the muscularis externa), middle (mixed smooth and skeletal muscle) and lower (entirely smooth muscle) portions. Slide UCSF 226 is from the upper 1/3; slides 126 and 153 are from the middle 1/3; and slide 155 is from the lower 1/3 (at the esophageal-cardiac junction). The esophageal epithelium [example] is the non-keratinized stratified squamous type and is supported by a connective tissue lamina propria. Note the presence of isolated lymphoid nodules [example] and scattered leukocytes in the lamina propria. A rather thick layer of longitudinally arranged smooth muscle fibers form the muscularis mucosae [example]. The connective tissue of the submucosa consists of mostly collagenous fibers with some elastic fibers and varying amounts of fat as well as submucosal sero-mucous glands which can be readily observed in both slide 126 [example] and slide 153 [example] (those in slide 155 are not very well preserved).
In the upper esophagus, as shown in Slide UCSF 226, the muscularis externa consists of both inner and outer layers of skeletal muscle only. In the middle esophagus, the muscularis externa contains a mixture of skeletal and smooth muscle as seen in slide 126 [example], whereas in the lower esophagus only smooth muscle is found as seen in slide 155 [example]. Present in all regions of the esophagus (upper, mid, and lower) is the myenteric (Auerbach’s) plexus [example] between the two layers of the muscularis externa (W pg 267, 14.3). For most of its extent, the esophagus is retroperitoneal, so its outermost layer consists of a connective tissue adventitia which merges with the adjacent connective tissue associated with nearby structures (such as the trachea as shown in slide 126). Below the diaphragm, however, the esophagus is suspended within abdominal cavity and is therefore covered by a connective tissue serosa as shown in slide 155.
|
What is the MOST LIKELY diagnosis?
ANSWER
129-1. What is the least important contributory risk factor for this neoplasm?
- Alcohol and tobacco abuse
- Barrett’s esophagus
- Human papilloma virus
- Fungi, nitrates, nitrosamines in food
ANSWER
129-2. The most important risk factor for adenocarcinoma of the esophagus is:
- Alcohol and tobacco abuse
- Barrett’s esophagus
- Human papilloma virus
- Fungi, nitrates, nitrosamines in food
ANSWER
CASE NUMBER 154
[Aperio ImageScope] [Aperio WebScope]
Clinical History: A 64-year-old man who had smoked two packs a day for 40 years complained of hoarseness and throat pain. A laryngectomy was performed.
Image Gallery:
(Summary of Gross Findings - click here)
An ulcerated tumor involved the left true and false vocal cords and extended across the midline.
|
(Summary of Microscopic Findings - click here)
The mucosa is partially columnar, representing the ventricular mucosa. There is a transition to squamous mucosa with marked nuclear pleomorphism. The abnormal squamous cells extend into the underlying stroma where the cells keratinize. Focal necrosis and an inflammatory infiltrate are present.
|
(Review Normal Histology - click here)
Webslide 0307_T: Larynx, sagittal section, H&E
[Aperio ImageScope] [Aperio WebScope] [backup WebScope]
The larynx is a passageway for air between the oropharynx and trachea which also functions in the production of sound. It is lined by pseudostratified columnar epithelium (see left hand side of the slide), stratified squamous epithelium (covering the vocal cords near the middle of the slide), and stratified columnar epithelium between these epithelial types. Seromucous glands are present underneath the epithelium on both sides of the slide. Identify the vocal cord as a mucoal fold covered by stratified squamous epithelium and containing abundant skeletal muscle. Notice the cartilage framework, some of which has partially ossified as commonly occurs with age.
|
154-1. The histological type of this tumor is BEST described as:
- Adenocarcinoma
- Adenosquamous carcinoma
- Squamous cell carcinoma
- Small cell neuroendocrine carcinoma
- Large cell undifferentiated carcinoma
ANSWER
154-2. Which of the following risk factors is MOST STRONGLY associated with this disease?
- Smoking
- Copper deficiency
- Hepatitis B virus
- Aniline dye
- NONE of the above
ANSWER
CASE NUMBER 31
[Aperio ImageScope] [Aperio WebScope]
Clinical History: This 45-year-old man had been well until he was awakened by chest pain that radiated to both arms and neck and was associated with diaphoresis. His blood pressure was 160/110. He was treated with diuretics (Lasix), but he continued to gain weight. Two days after the onset of the chest pain he had a cardiac arrest and died.
Image Gallery:
(Summary of Gross Findings - click here)
The heart was slightly enlarged weighing 460gms. There was severe atherosclerosis of all the major coronary arteries with a recent thrombotic occlusion of the proximal left anterior descending coronary artery. A recent transmural infarct was present in the left ventricle that involved the interventricular septum and the papillary muscle.
|
(Summary of Microscopic Findings - click here)
The slide includes a transmural section of the left ventricle. Nearly the entire section is involved by infarct. However, there is a thin rim (5 to 10 cell layers) of endocardial myocytes which have survived because of diffusion of oxygen and nutrients from the ventricular cavity. Other viable myocytes can be found around larger blood vessels within the section. The intense hypereosinophilia of the necrotic myocytes can best be appreciated by comparing the thin rim of lighter staining subendocardial myocytes with the deeper cells. Note also the karyolysis that is characteristic of coagulation necrosis. In some areas there is little inflammatory response. This observation is explained by microvascular necrosis which does not allow access of circulating leukocytes to these areas. In other areas, especially in the epicardial half of the infarct, there is an intense acute inflammatory response. Many intact neutrophils can be seen. In addition, there are many nuclear fragments from lysed neutrophils. Macrophage activity is not evident. These features of the inflammatory response indicate that the infarct was approximately three to four days old. Note also that the inflammation extends to the epicardial surface and that there are deposits of fibrin on the epicardium. This is called fibrinous pericarditis. The granular grey material seen within some blood vessels is barium sulfate, which was injected to permit post-mortem study of the coronaries by radiography.
|
(Review Normal Histology - click here)
Norm No. 13 Heart
[ImageScope] [WebScope]
Normal heart tissue sections demonstrate no evidence of fibrosis or hemorrhage. Cardiac myocytes have moderately sized centrally located nuclei. Normal myocytes are not brightly eosinphilic. Normally no inflammation is seen. Normal cardiac myocytes do not show hypertrophy.
|
What is the MOST LIKELY diagnosis?
ANSWER
31-1. The event MOST LIKELY associated with this patient’s problem was:
- Occlusion of a coronary vein
- Occlusion of a coronary artery
- Stabbed with ice pick
- Broken heart
ANSWER
31-2. What microscopic feature BEST describes what happened to the nuclei of the dead myocytes?
- Pyknosis
- Karyorrhexis
- Karyolysis
- Apoptosis
ANSWER
31-3. What molecular events led to the increase eosin staining of the dead myocytes?
- Loss of ribosomes
- Protein denaturation
- Protein synthesis
- A & B
ANSWER
31-4. What microscopic feature in this patient indicates that this infarct is at least 24 hours old?
- Coagulation necrosis & loss of nuclei
- Wavy fibers
- Macrophage infiltrate
- Granulation tissue
ANSWER
31-5. What microscopic feature is most indicative of reperfusion of ischemic myocardium with irreversible injury?
- Necrosis with contraction bands
- Endothelial swelling
- Wavy fibers
- Hypereosinophilic cytoplasm
ANSWER
31-6. What myocardium is the most vulnerable to ischemic injury in hypovolemic shock?
- Subepicardial, left ventricle
- Mid-myocardial, left ventricle
- Subendocardial, left ventricle
- Subendocardial, right ventricle
ANSWER
ENVIRONMENTAL PATHOLOGY Review Items
Key Vocabulary Terms (click here to search any additional terms on Stedman's Online Medical Dictionary)
LEARNING OBJECTIVES
Absolutely critical information you must know to practice medicine is in bold font.
Important information that will be needed for routine patient care is in regular font.
Information about less common diseases that you may encounter in clinical practice and that will probably appear on examinations is in italics
- Discuss the following in terms of role in indoor vs. outdoor air pollution:
- List the various substances found in cigarette smoke and their health effects.
- Discuss the effects and clinical significance of:
- active tobacco smoke
- passive (sidestream) tobacco smoke
- smokeless tobacco
- Outline the basic pathogenesis of pneumoconioses.
- Compare and contrast the following pneumoconiosis in terms of types of occupational exposure, pathogenesis and clinical course
- coal workers' pneumoconiosis
- silicosis
- asbestosis
- berylliosis
- Compare coal workers' pneumoconiosis with simple asymptomatic anthracosis.
- Discuss Caplan syndrome in relation to coal workers' pneumoconiosis, asbestosis, and silicosis.
- Describe the ways in which the following factors influence chemical injuries:
|
- physical properties of chemical
|
|
|
|
- nutritional status of patient
|
|
|
|
|
- Describe the ways in which the following factors influence chemical injuries:
|
|
|
|
|
|
|
|
|
|
|
|
|
- organochlorine insecticides
|
|
- organophosphate insecticides
|
- Discuss ethanol in terms of:
- effects ethanol on society
- blood alcohol levels and their effects
- metabolism and systemic effects of:
- acute alcohol ingestion
- chronic ethanol abuse
- Discuss the following:
- fetal alcohol syndrome
- association of ethanol with cancer
|