The CSF Gram stain showed Gram-positive diplococci, subsequently growing S. pneumoniae. A peripheral blood culture revealed the same organism.
|
Clinical History: The clinical history will be presented by Infectious Disease faculty. The image below corresponds with diganostic studies carried out while the patient was admitted to the hospital. Image Gallery:
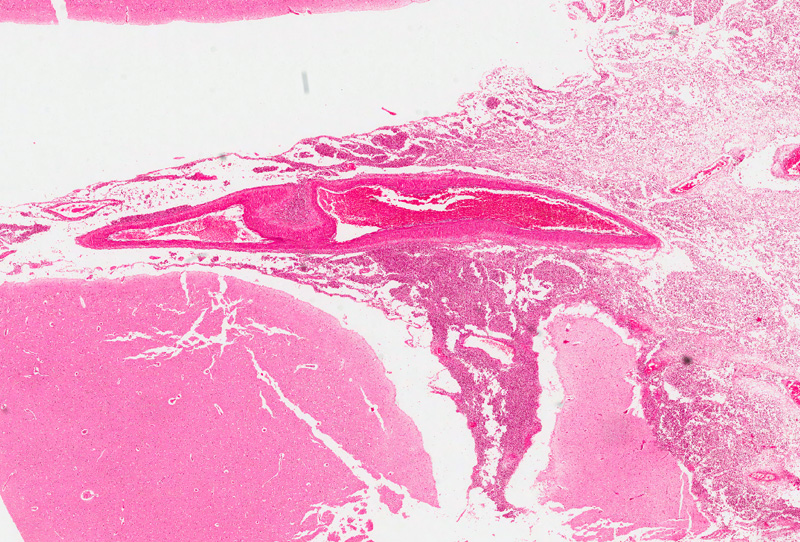
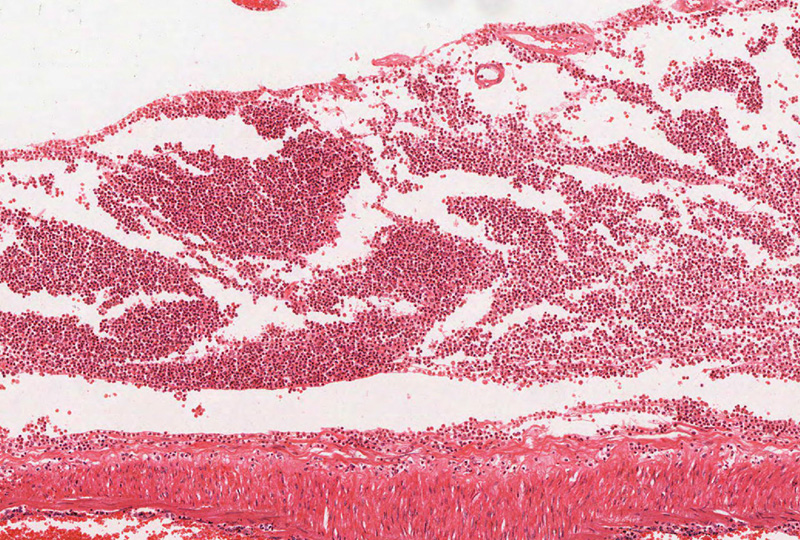
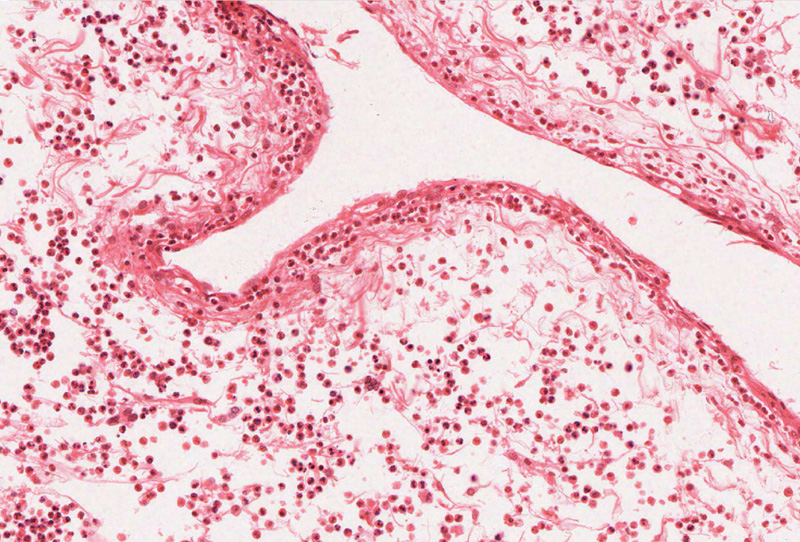
Clinical history (conclusion): Despite aggressive therapy, the patient dies. Gross and microscopic images from specimens obtained at autopsy are shown. Virtual Slide (slide courtesy of IndianaU): [ImageScope] [WebScope] Image Gallery:
|
||