CASE NUMBER 544
Slide 0544_H&E.svs [DigitalScope]
Slide 0544_Tau.svs [DigitalScope]
--Click here to view a video debrief regarding the pathology findings presented in this case--
Clinical History: A 78-year-old retired woman with a history of well-controlled hypertension was brought in by her son after she became lost taking her grandchildren home from the park. She was previously independent and is a retired professor but after the death of her husband 4 years ago, moved in with her son’s family. The patient has no specific complaints though her son reports several times she thought she was still in her own home, which he attributed to grief. More recently (last 1-2 years) she has had trouble with grocery shopping and taking medications as prescribed. She voluntarily stopped driving six months ago.
Vital signs were notable for a BP of 143/90. Neurological exam revealed a frail elderly woman who was cooperative with the examiner. She was alert and oriented to self and year but not date or location. She was unable to name the president or vice president. Speech pattern was tangential but fluent. Confrontational naming was normal. She was unable to count backwards by 7, and she was able to recall 3 of 5 words immediately after hearing them, but could not remember them after 5 minutes. The remainder of her neurological and general medical exam was normal.
Differential diagnosis:
544-1. What is the differential diagnosis?
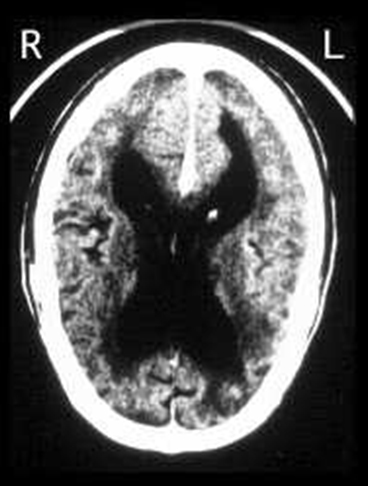
MRI of the brain revealed generalized atrophy, somewhat more prominent in the L > R temporoparietal region, and enlargement of both lateral ventricles. There were minimal scattered T2/FLAIR hyperintensities consistent with microvascular ischemic disease. Laboratory studies for thyroid function and vitamin B12 were normal.
Radiology image questions:
- Describe the radiographic findings. What is the most likely cause of this appearance?
Over the next 5 years, her cognition progressively deteriorated, and she began to have trouble swallowing, with recurrent episodes of aspiration pneumonitis requiring hospitalization. A goals of care discussion was initiated between patient and family, and all parties agreed that she would not want a PEG tube and would benefit from a transition to palliative care and hospice. The patient died three weeks later.
Image Gallery:
|
Review Neuroradiology |
Review Cerebral Cortex Histology
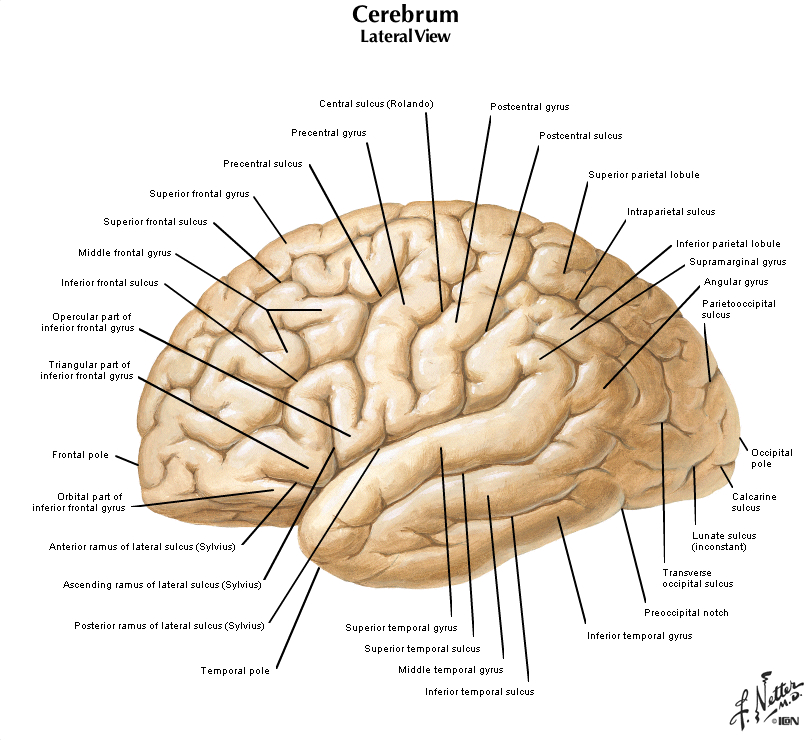
Cerebrum
Slide 76 (cerebrum, luxol blue/cresyl violet) [DigitalScope]
Slide 76b (toluidine blue & eosin) [DigitalScope]
The cerebral cortex is loosely stratified into layers containing scattered nuclei of both neurons and glial cells. Examine the layered organization of the cerebral cortex using slide 76 stained with luxol blue/cresyl violet [ORIENTATION] (which stains white matter tracts and cell bodies) or toluidine blue and eosin [ORIENTATION] (TB&E, toluidine blue stains the nuclei and RER of cells whereas eosin stains membranes and axon tracts). Typically one or more sulci (infoldings) will extend inward from one edge of the section. Examine the gray matter on each side of the sulcus using first low and then high power. Neurons of the cerebral cortex are of varying shapes and sizes, but the most obvious are pyramidal cells. As the name implies, the cell body is shaped somewhat like a pyramid, with a large, branching dendrite extending from the apex of the pyramid toward the cortical surface, and with an axon extending downward from the base of the pyramid. In addition to pyramidal cells, other nuclei seen in these sections may belong to other neurons or to glial cells also present in the cortex. You may be able to see subtle differences in the distribution of cell types in rather loosely demarcated layers. There are 6 classically recognized layers of the cortex:
- Outer plexiform (molecular) layer: sparse neurons and glia
- Outer granular layer: small pyramidal and stellate neurons
- Outer pyramidal layer: moderate sized pyramidal neurons (should be able to see these in either luxol blue or TB&E-stained sections)
- Inner granular layer: densely packed stellate neurons (usually the numerous processes aren’t visible, but there are lots of nuclei reflecting the cell density)
- Ganglionic or inner pyramidal layer: large pyramidal neurons (should be able to see these in either luxol blue or TB&E-stained sections)
- Multiform cell layer: mixture of small pyramidal and stellate neurons
Pyramidal cells in layers III and V tend to be larger because their axons contribute to efferent projections that extend to other regions of the CNS –pyramidal neurons in layer V of motor cortices send projections all the way down to motor neurons in the spinal cord!
Deep to the gray matter of the cerebral cortex is the white matter that conveys myelinated fibers between different parts of the cortex and other regions of the CNS. Be sure you identify the white matter in both luxol blue and TB&E-stained sections, as it will appear differently in these two stains. Review the organization of gray and white matter in cerebral cortex vs. spinal cord.
|
Review Hippocampus and Dentate Gyrus Histology
NP004N hippocampal region, coronal section, luxol blue [DigitalScope]
This coronal section includes the hippocampus (hippocampus = sea horse), dentate gyrus, and adjacent temporal lobe gyrus (entorhinal cortex). Above the temporal (ventral or inferior) horn of the lateral ventricle the lateral geniculate nucleus is present. Lateral to this structure is the tail of the caudate. The medial surface of the section is the posterior portion of the thalamus and a small portion of the cerebral peduncle. Look at the margins of the ventricle at higher magnification and note that it is entirely lined by ependymal cells. Just medial (to the right) of the tail of the caudate, note the choroid plexus, which consists of highly convoluted and vascularized villi covered by ependymal cells which are specialized for the production of cerebrospinal fluid, or CSF.
The hippocampus and dentate gyrus function in what is known as the "limbic system" to integrate inputs from many parts of the nervous system into complicated behaviors such as learning, memory, and social interaction beyond the scope of what can be described here. For now, focus just on the morphology of these regions and observe the presence of three distinct layers rather than the six layers found in the cerebral cortex (evolutionarily speaking, the three-layered organization is considered to be "older," so this type of cortex is also known as "archicortex"). In the hippocampus [ORIENTATION], observe:
- ("1" in the orientation figure) a polymorphic layer containing many nerve fibers and small cell bodies of interneurons,
- ("2" in the orientation figure) a middle pyramidal cell layer containing hippocampal pyramidal cells, and
- ("3" in the orientation figure) a molecular layer containing dendrites of the pyramidal cells.
In the dentate gyrus [ORIENTATION], observe:
- ("4" in the orientation figure) a polymorphic layer containing nerve fibers (known as "mossy fibers") and cell bodies of interneurons,
- ("5" in the orientation figure) a middle granule cell layer containing the round, neuronal cell bodies of dentate granule cells , and
- ("6" in the orientation figure) a molecular layer containing dendrites of the granule cells.
|
Summary of CT Findings
There is a dramatic loss of parenchyma, manifested here by cortical atrophy and marked enlargement of the lateral ventricles (called hydrocephalus ex vacuo).
|
Summary of Gross Findings
Patient's brain (left) with a normal brain (right). There is extensive widening of the sulci and narrowing of gyri in the patient's brain, indicative of substantial loss of brain parenchyma. (The color difference is due to the meningeal covering of the normal brain.)
|
Summary of Microscopic Findings
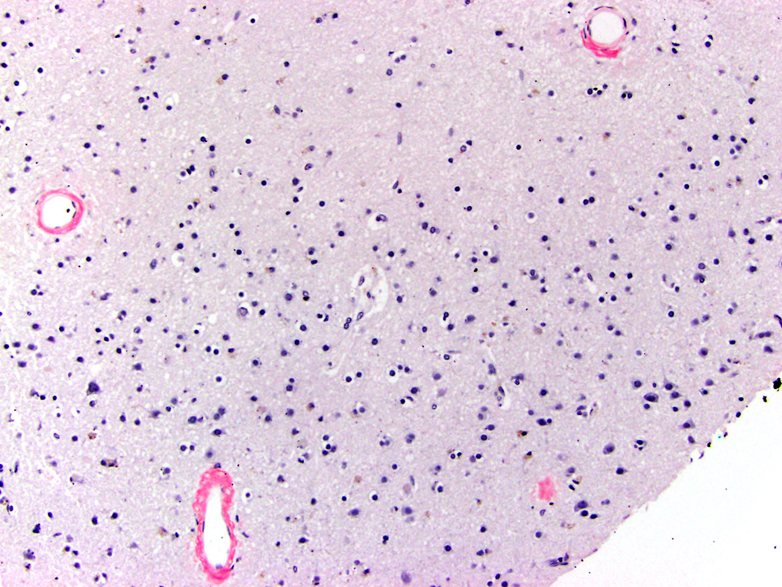
On H&E stain, there are multiple ghost neurons with residual neurofibrillary tangles as well as viable neurons with tangles in the hippocampus. Overall, there is a decrease in viable neurons. In addition, there are scattered plaques. On Congo Red stain, amyloid can be seen in vessel walls. Tau immunostaining highlights many neurofibrillary tangles and plaques.
|
Gross image questions:
VM image questions:
- On an annotated image, identify a neurofibrillary tangle and a plaque. Why is there diffuse staining with tau on immunohistochemistry?
- What does the Congo red stain demonstrate?
544.2 What are plaques and tangles and how do they correlate with symptoms?
--ANSWER--
544.3 How does Ab contribute to the pathogenesis of AD?
--ANSWER--
544.4 How does tau contribute to the pathogenesis of AD?
--ANSWER--
544.5 What are some conditions that are associated with an increased risk of AD and why?
--ANSWER--
|