Clinical History: This 57-year-old male presented with back pain, lytic lesions in many bones, Bence-Jones proteinurea and marked plasmacytosis of the marrow. Some therapeutic response was obtained with chemical agents and X-radiation. Death followed pneumonia and sepsis.
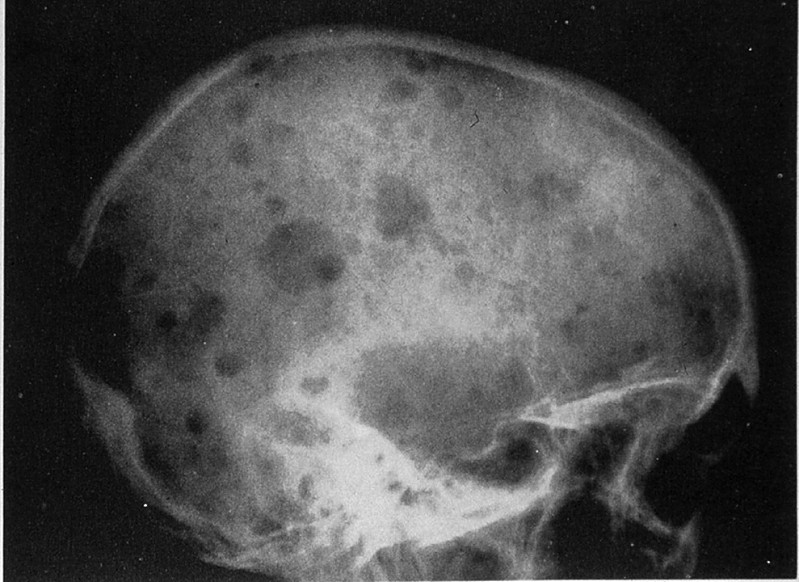
Many of the bones contained poorly delineated, soft gelatinous red tumor masses of various dimensions. Plain film of the skull shows sharply punched out bone lesions.
The marrow is heavily infiltrated with plasma cells which vary in degree of maturation. Islets of normoblasts are present, but granulocytes and megakaryocytes are markedly decreased. There is considerable loss of trabecular and cortical bone.
A thin layer of compact/dense bone borders this section, with internal cancellous/spongy bone. The spaces between bony spicules are filled with hematopoietic cells. Not the large numbers of (round, empty) fat cells present within the marrow space. The fat is lost during processing into paraffin sections. Megakaryocytes can be readily identified, since they are approximately 5-fold larger than most bone marrow cells and contain strongly eosinophilic cytoplasm and multiple nuclei.
(slide and description courtesy of Dr. Laura Hale, Duke PATHOL725 course director)
413-1. This following is a common feature of this neoplasm:
Presents with Waldenstrom macroglobulinaemia
Proliferation and survival of neoplastic cells are dependent on IL-1
Most common site of bone involvement is the epiphyses of long bones
May be associated with excretion of Bence-Jones proteins
The normal lymph node architecture is completely destroyed. In its place are thick bands of collagen, separating islands of lymphoid tissue. In some of these nodules, there is a mixed infiltrate consisting of lymphocytes, eosinophils, some neutrophils and plasma cells, and numerous large cells with highly pleomorphic nuclei. Nuclei are frequently multi lobulated but classic binucleate Reed-Stemberg cells are uncommon. Many cells are so-called "lacunar variants", with nuclei which have artefactually shrunken away from their cytoplasmic borders, leaving a clear space than can often easily be appreciated at low power.
The lymph node contains a cortex which includes the lymphoid follicles and a medulla which is looser tissue containing the lymphatic channels and blood vessels.
Clinical History: A 51-year-old male had a "neurogenic bladder", caused by a spinal cord tumor. He had multiple bladder infections which were treated with antibiotics. He had surgery to remove the tumor. Postoperatively, he developed fever and costovertebral angle tenderness which did not respond to antibiotics. He expired and an autopsy was performed.
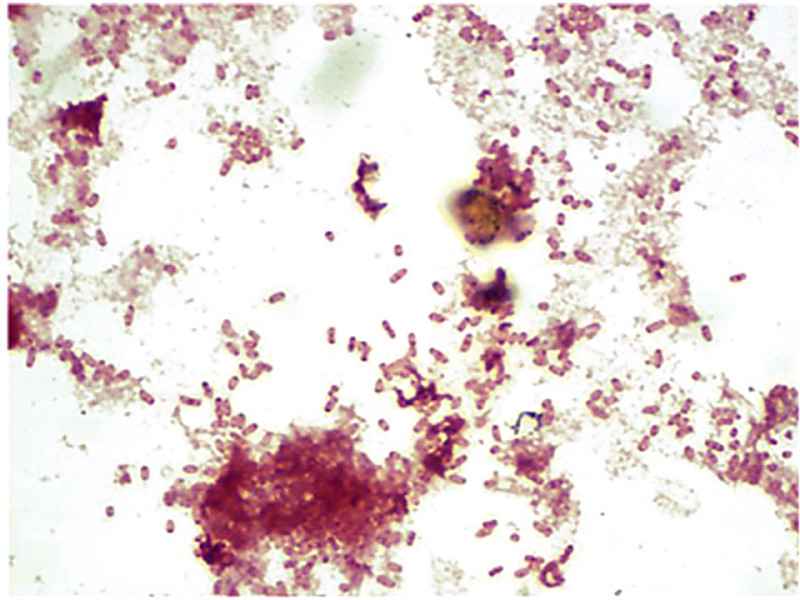
The organism grew on blood agar and on MacConkey agar. Gram stain of a blood culture showed gram negative rods. A catheterized urine specimen was obtained before death. Greater than 100,000 colonies of E. Coli were cultured. The bladder was distended, with a thickened, trabeculated wall. There was a bilateral hydroureter and hydronephrosis. The left kidney was swollen, and the cut surface showed soft foci of yellow streaks extending toward the pelvis.
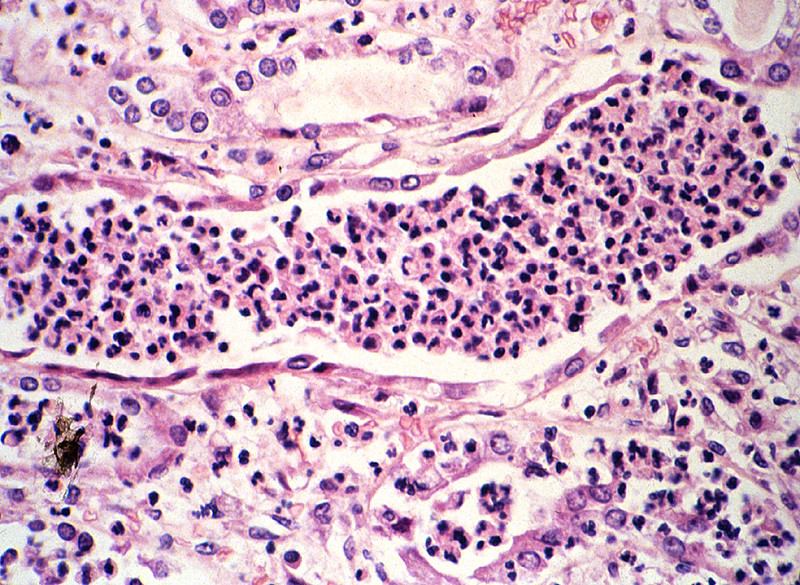
Naked eye examination of the slide reveals dark streaks extending from the outer cortex to the inner medulla. Microscopically these are foci of acute inflammation, including necrosis and hemorrhage, with masses of polymorphonuclear leukocytes that are also found in many tubules.
The kidney excretes soluble waste from the body and controls electrolyte balance. It consists of the cortex and the medulla. Within the outer cortex, glomeruli with delicate capillary loops are seen. The basement membrane is thin and without inflammation or thickening. Bowman’s capsule that surrounds the glomerulus is thin. The interstitium demonstrates no evidence of inflammation or fibrosis. In the areas between the glomeruli, tubules and arterioles are seen. The tubules are intact. The vessels exhibit no narrowing or wall thickening. The inner medulla of the kidney contains only tubules and blood vessels. Larger arteries and veins are located at the interface between cortex and medulla.
Clinical History: A 65-year-old woman had experienced increasing malaise with nocturia and polyuria for the past year. Her blood pressure was 170/95. Urinalysis showed 1+ proteinuria. Serum BUN and creatinine were elevated. She developed worsening renal failure and died of pneumonia.
The kidneys are small with irregular and coarse U-shaped corticomedullary scars overlying dilated, blunt, deformed calyces. Extensive scarring is noted at the hilum of each kidney. Evidence of hydronephrosis and cortical thinning is also observed.
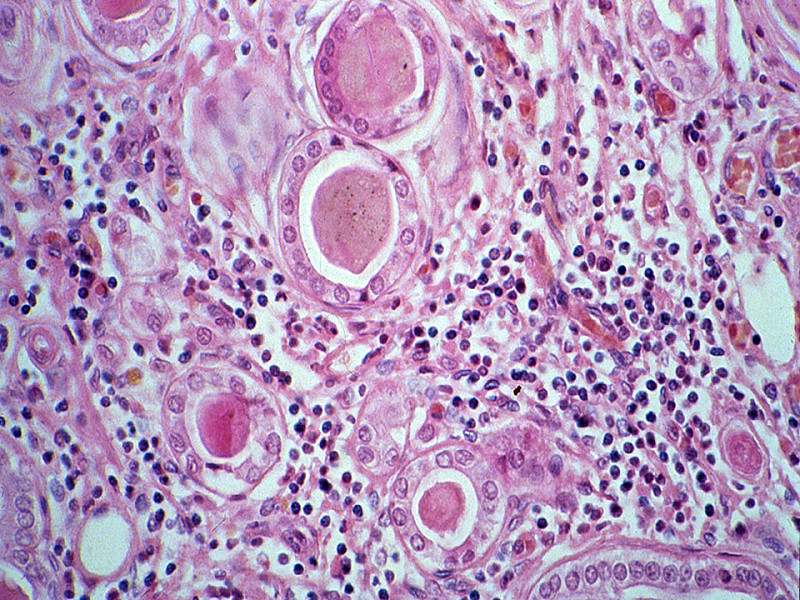
Interstitial tissue shows prominent infiltration by lymphocytes and plasma cells, and occasional polymorphonuclear neutrophils; irregular fibrous scars and peri-glomerular fibrosis. Tubules are dilated, many filled with eosinophilic casts giving the region a "thyroid-like" appearance. A few tubules contain polymorphonuclear neutrophils, indicating that this is an active exacerbation of a chronic pyelonephritis. Arteries are markedly thickened, with intimal proliferation resulting in narrowing of the lumen. Many arterioles show hyaline changes in their walls. Most glomeruli are replaced by fibrous tissue. A few are surprisingly normal in appearance with intact capillaries. There is a prominent peri-glomerular fibrosis in many regions with a thick rim of fibrous tissue circling the outside of Bowman's capsule.
The kidney excretes soluble waste from the body and controls electrolyte balance. It consists of the cortex and the medulla. Within the outer cortex, glomeruli with delicate capillary loops are seen. The basement membrane is thin and without inflammation or thickening. Bowman’s capsule that surrounds the glomerulus is thin. The interstitium demonstrates no evidence of inflammation or fibrosis. In the areas between the glomeruli, tubules and arterioles are seen. The tubules are intact. The vessels exhibit no narrowing or wall thickening. The inner medulla of the kidney contains only tubules and blood vessels. Larger arteries and veins are located at the interface between cortex and medulla.
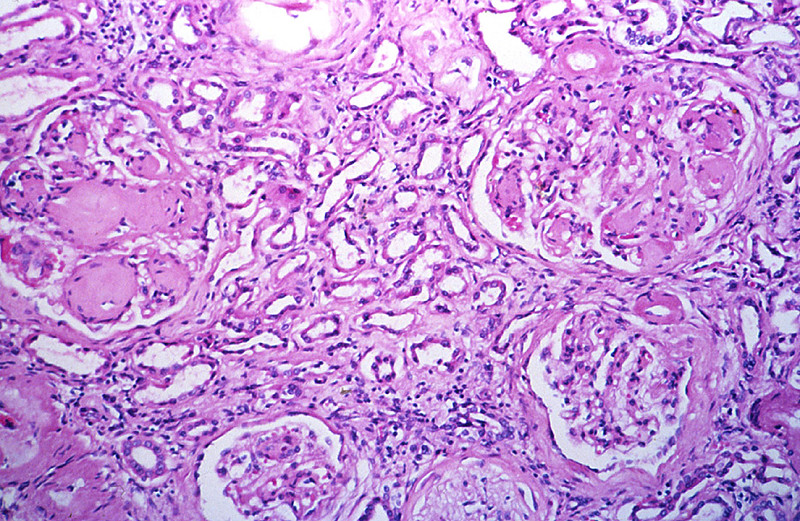
Clinical History: This 55 year old female first came to medical attention when she complained of frequent urination, increased thirst and weight loss at age 15. Insulin dependent diabetes was diagnosed. She developed proteinuria at age 20. Her disease progressed until she became dialysis dependent at age 45. She expired due to pneumonia after a below knee amputation
There are glomerular lesions consisting of diffuse and nodular glomeroslerosis. Nodular glomerulosclerosis or Kimmelstiel-Wilson lesions are ball-like deposits of PAS positive material which contain trapped mesangial cells. These occur in 15-30% of long time diabetics and are virtually pathognomonic of the disease. Diffuse glomeruloslerosis usually appears as global sclerosis of the glomerular tuft. Chronic pyelonephritis, arterio and arteriolo nephrosclerosis as seen here are also typical findings in diabetic kidneys.
The kidney excretes soluble waste from the body and controls electrolyte balance. It consists of the cortex and the medulla. Within the outer cortex, glomeruli with delicate capillary loops are seen. The basement membrane is thin and without inflammation or thickening. Bowman’s capsule that surrounds the glomerulus is thin. The interstitium demonstrates no evidence of inflammation or fibrosis. In the areas between the glomeruli, tubules and arterioles are seen. The tubules are intact. The vessels exhibit no narrowing or wall thickening. The inner medulla of the kidney contains only tubules and blood vessels. Larger arteries and veins are located at the interface between cortex and medulla.
Absolutely critical information you must know to practice medicine is in bold font. Important information that will be needed for routine patient care is in regular font. Information about less common diseases that you may encounter in clinical practice and that will probably appear on examinations is in italics
List the clinical criteria for diagnosis and pathology
Discuss the proper use of the following laboratory tests in the evaluation of urinary tract disease and interpret abnormalities of these parameters in clinical context:
creatinine
urea (blood urea nitrogen, BUN)
urinalysis
Discuss the clinical and pathologic features of the following congenital renal anomalies:
Absolutely critical information you must know to practice medicine is in bold font. Important information that will be needed for routine patient care is in regular font. Information about less common diseases that you may encounter in clinical practice and that will probably appear on examinations is in italics
Define and state the significance of each of these peripheral blood smear findings:
Compare and contrast the reporting of leukocyte differential counts as relative percentages vs. absolute numbers, in terms of the advantages and disadvantages of each system.
Describe the proper mode of submission of a lymph node biopsy to the surgical pathology laboratory for workup of a suspected lymphoproliferative disorder.
Define, state the significance of, and identify in a microscopic section of a lymph node or extranodal site of involvement each of the following: