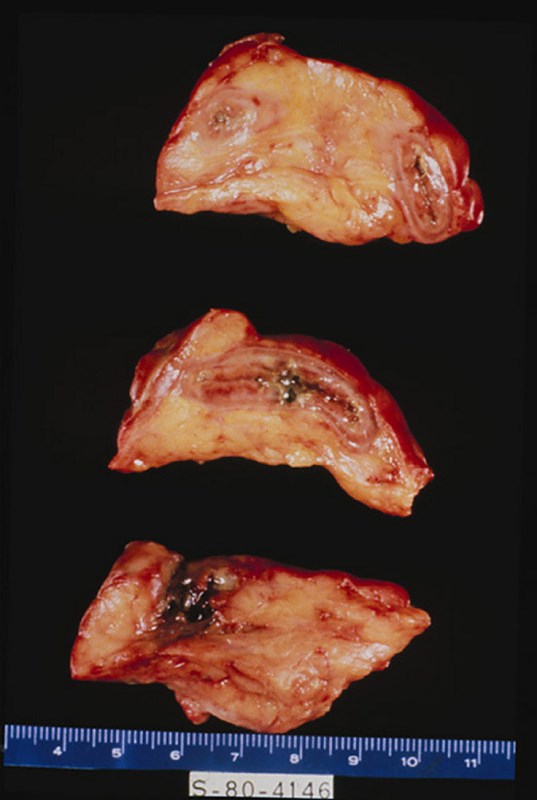
Clinical History: This patient was a 54-year-old male who had a long history of peptic ulcer disease. A portion of the stomach was removed. Medical management is more common today.
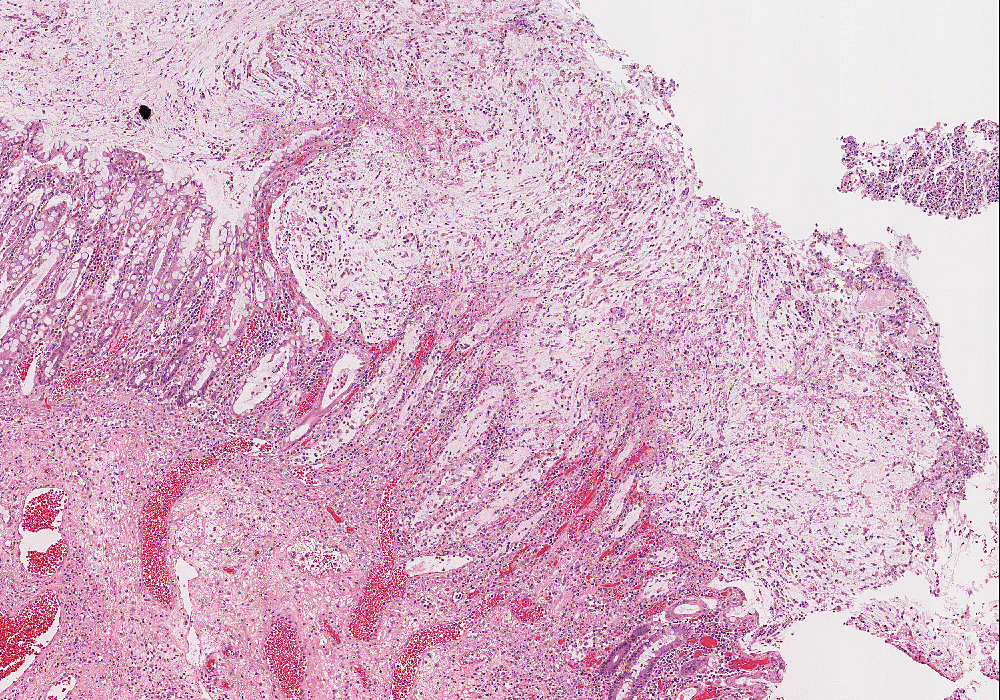
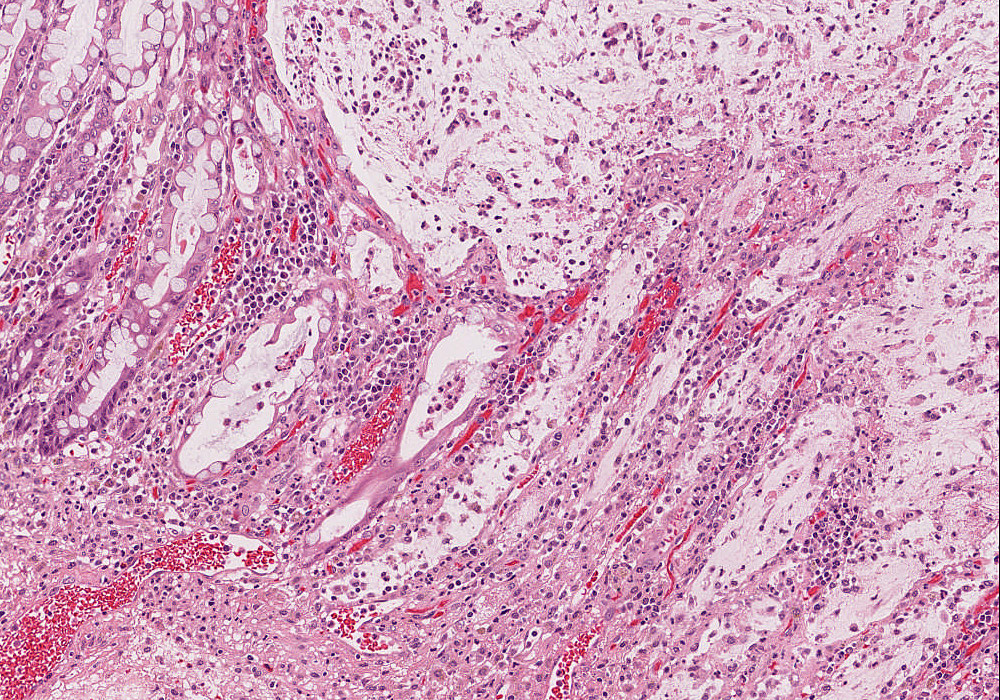
Microscopic sections show a portion of antral/pyloric stomach. A large ulcer and the accompanying response have replaced all layers of the stomach mucosa and wall. Three layers may be distinguished in the bed of the ulcer. The innermost one is composed of necrotic debris and fibrino-purulent exudate in which bacteria and yeast are present. The middle layer is a zone of granulation tissue made up of small vessels and acute and chronic inflammation. The deepest portion of the ulcer is made up of fibrous scar. Some of the arteries in the scar tissue may show sclerosis. The mucosa adjacent to the ulcer shows acute and chronic gastritis.
The normal gastric mucosa of the fundus contains superficial fovea arranged in leaf like fronds and deeper gastric glands. The foveolar cells secrete mucin. The gastric glands include mucous cells, parietal cells, chief cells and enteroendocrine cells.
240-1. This patient’s lesion is best characterized as:
Clinical History: An 18-year-old female had nausea, vomiting, periumbilical and lower abdominal pain, shaking chills and fever beginning two days ago. The WBC count was 21,900. Physical examination revealed local tenderness and rigidity with rebound pain in the lower abdomen. A surgical procedure was performed.
The appendix was swollen, dark red, hemorrhagic, and covered by gray-yellow exudate. Serial cross-sections revealed a distended lumen containing hemorrhagic material and a fecalith, which apparently obstructed the lumen.
Portions of the mucosa are ulcerated, necrotic and heavily infiltrated with neutrophils. This acute inflammation and necrosis extends throughout the entire thickness of the wall and the serosa. In the lumen of the appendix there is pus and a fecalith.
The appendix is a tubular organ with a lumen which is lined by mucin secreting columnar epithelium. Although there are generally numerous lymph nodules in the lamina propria and submucosa under normal conditions, there is no evidence of acute inflammation. The submucosa and muscle layers are unremarkable, and there is no inflammation of the serosa.
Clinical History: This 73-year-old female presented with right upper quadrant pain and elevated WBC count. Physical exam revealed right upper quadrant tenderness. Ultrasound examination of the gallbladder revealed gallstones. A cholecystectomy was performed.
The gallbladder contained composite gallstones with a yellow to black appearance. Gallstones consist of a mixture of cholesterol, bilirubin, and calcium. Pure stones are uncommon, though jet black bilirubin stones suggest chronic hemolysis. The stones shown here are squared off (faceted) because they sat together. If gallstones obstruct the biliary duct, acute cholecystitis may develop.
The gallbladder mucosa is acutely inflamed with many neutrophils in the epithelium and lamina propria. The epithelium is reactive with enlarged nuclei and abundant eosinophilic cytoplasm and ulcerated in some areas. There is hemorrhage and fibroblastic proliferation throughout the wall. Chronic cholecystitis is evidenced by plasma cells in the mucosa and Rokitansky-Aschoff sinuses which are diverticular invaginations of mucosa in the gallbladder wall. No tumor is seen.
The gall bladder is a distensible sac with extensive folds of mucosa that extend into the lumen. The mucosa consists of a tall, simple columnar epithelium and its underlying connective tissue (constituting a laminapropria). Note that there is NO SUBMUCOSA. The muscularis consists of scattered bundles of smooth muscle. Deep to the muscularis is an adventitia consisting of rather dense connective tissue that binds the gall bladder to the liver. Where the surface of the gall bladder faces the abdominal cavity there is a serosa.
Clinical History: This 51-year-old white female had bloody diarrhea which responded to immunosupressant therapy for many years. Her symptoms progressed and portion of the colon was removed.
The mucosa showed an area of edema and hyperemia distally. This was sharply demarcated from the remainder of the colon. A superficial mucosal lesion was noted.
This section shows fulminant ulcerative colitis with areas of ulceration extending into the submucosa and also some areas of hemorrhage. While deep ulceration is seen, there is no fissuring necrosis, fibrous expansion of the submucosa, or transmural chronic inflammation, which differentiates this lesion from Crohn's disease. The base of the ulcerated area is covered by necrotic debris and fibrinopurulent or sanguinous exudate. Glands are distorted in shape, infiltrated by neutrophils, and lined by regenerating epithelium.
The colon is lined by glandular epithelium with numerous mucin secreting goblet cells. The epithelium is infolded into straight tubular glands of uniform diameter to increase the surface area available for secretion and absorption.
Clinical History: This 39-year-old male had a history of non-healing rectal fistula and a long standing history of enteritis. There was bloody and mucous diarrhea. Part of the colon was resected due to bowel obstruction.
The colon showed extensive ulcerations separated by pedunculated areas of hypertrophic mucosa. The intestinal wall was swollen and edematous. The serosa was thickened with fibrous adhesions.
A broad area of ulceration extends into the submucosa. The surface of the ulcer is covered by fibrinopurulent exudate overlying granulation tissue. Neutrophils infiltrate glands in the adjacent mucosa, some of which are lined by regenerating epithelium. A few crypts are distorted in shape. These features differ little from those seen in ulcerative colitis (Case No. 111). However, this section also shows transmural chronic inflammation in the form of lymphoid aggregates and granulomatous inflammation.
The colon is lined by glandular epithelium with numerous mucin secreting goblet cells. The epithelium is infolded into straight tubular glands of uniform diameter to increase the surface area available for secretion and absorption.
The liver weighed 1800 grams. The entire organ was uniformly composed of nodules about 0.5 cm in diameter, each surrounded by fibrous tissue. The organ was jaundiced and firm.
The usual architecture present in the liver has been completely disrupted by the bands of connective tissue. In these bands one sees chronic inflammatory cells, mainly lymphocytes and other mononuclear cells. There is some proliferation of the bile ductules.
The liver is the organ that metabolizes nutrients received from the digestive tract. These nutrients and processed by tissue hepatocytes which are large polygonal cells. The hepatocyes are separated by portal triads. The triads consist of an artery, a vein and a bile duct. The bile duct is lined by cuboidal epithelium. The artery has a muscular wall and a flat endothelial lining. The sinuses are well defined and contain a small amount of blood.
The liver architecture is completely replaced by fibrosis and regenerative nodule formation. In the broad fibrous bands separating regenerative nodules, there is abundant proliferation of bile ductules. The most striking feature of this liver is the severe cholestasis. Bile is seen in ducts, ductules and dilated cannuliculi. In scattered foci, it breaks into the liver parenchyma forming "bile lakes".
The liver is the organ that metabolizes nutrients received from the digestive tract. These nutrients and processed by tissue hepatocytes which are large polygonal cells. The hepatocyes are separated by portal triads. The triads consist of an artery, a vein and a bile duct. The bile duct is lined by cuboidal epithelium. The artery has a muscular wall and a flat endothelial lining. The sinuses are well defined and contain a small amount of blood.
In the right lobe of the liver there was a circumscribed, dark red, spongy mass 4 cm in size. In the center of the mass there was a gray, firm, fibrous core.
Inspection reveals a mass with many blood filled spaces. These are formed by anastomosing strands of connective tissue, partially hyalinized, lined by endothelial cells. Notice the subcapsular location of the tumor and its relationship to the liver parenchyma.
The liver is the organ that metabolizes nutrients received from the digestive tract. These nutrients and processed by tissue hepatocytes which are large polygonal cells. The hepatocyes are separated by portal triads. The triads consist of an artery, a vein and a bile duct. The bile duct is lined by cuboidal epithelium. The artery has a muscular wall and a flat endothelial lining. The sinuses are well defined and contain a small amount of blood.
Clinical history: A 45-year-old woman is being treated in the hospital for pneumonia complicated by septicemia. She has required multiple antibiotics and was intubated and mechanically ventilated earlier in the course. On day 20 of hospitalization, she has abdominal distention. Bowel sounds are absent, and abdominal radiograph shows dilated loops of small bowel suggestive of ileus. She has a low volume of bloody stool.
Absolutely critical information you must know to practice medicine is in bold font. Important information that will be needed for routine patient care is in regular font. Information about less common diseases that you may encounter in clinical practice and that will probably appear on examinations is in italics
Describe the formation of bile and explain abnormalities that could cause jaundice.
Discuss the clinical indications for the following laboratory tests:
Absolutely critical information you must know to practice medicine is in bold font. Important information that will be needed for routine patient care is in regular font. Information about less common diseases that you may encounter in clinical practice and that will probably appear on examinations is in italics
Compare and contrast the clinical and pathologic features of:
exocrine pancreatic insufficiency
endocrine pancreatic insufficiency
Discuss the clinical and pathologic features of cystic fibrosis.
Compare and contrast acute and chronic pancreatitis, in terms of:
etiologic/predisposing factors
pathogenesis
morphologic features
laboratory manifestations
clinical findings and course
complications
Compare and contrast the clinical and pathologic features of adenocarcinoma of the:
pancreatic head
pancreatic body/tail
ampulla of Vater
5. Discuss islet cell tumors of the pancreas, in terms of:
incidence
morphology
benignity vs. malignancy
immunohistochemical characteristics
endocrine function
clinical features and course
Discuss indications and complications of pancreatic islet cell transplantion.
Absolutely critical information you must know to practice medicine is in bold font. Important information that will be needed for routine patient care is in regular font. Information about less common diseases that you may encounter in clinical practice and that will probably appear on examinations is in italics
Describe the clinical and pathologic features of disorders of the esophagus:
pathogenesis, including genetic and molecular factors
morphology, including grading and staging criteria
clinical features and course
Contrast and compare clinical and pathologic features of carcinoma of right and left colon.
Discuss carcinoid tumors of the colon, rectum, and appendix, in terms of:
pathogenesis
morphology
clinical features (including extra-colonic manifestations)
course and prognosis
Describe the etiology, pathogenesis, and morphology of appendicitis
actinomycotic appendicitis. chronic suppurative appendicitis resulting from infection by Actinomyces israelii. acute appendicitis. acute inflammation of the appendix, usually resulting from bacterial infection, which may be precipitated by obstruction of the lumen by a fecalith; variable symptoms often consisting of periumbilical, colicky pain and vomiting may be followed by fever, leukocytosis, persistent pain, and signs of peritoneal inflammation in the right lower quadrant of the abdomen; perforation or abscess formation is a frequent complication of delayed surgical intervention. bilharzial appendicitis. appendicitis caused by deposition of the eggs of the blood fluke Schistosoma mansoni in the vermiform appendix. chronic appendicitis. fibrous adhesions, scarring, or deformity of the appendix following subsidence of acute appendicitis; fibrous obliteration of the distal lumen is not abnormal in older persons; term frequently used to refer to repeated mild attacks of acute appendicitis. focal appendicitis. acute appendicitis involving only part of the appendix, sometimes at the site of, or distal to, an obstruction of the lumen. foreign-body appendicitis. appendicitis caused by obstruction of the lumen of the appendix by a foreign substance, such as a particulate foreign body. gangrenous appendicitis. acute appendicitis with necrosis of the wall of the appendix, most commonly developing in obstructive appendicitis and frequently causing perforation and acute peritonitis. left-sided appendicitis. appendicitis occurring on the left side of the abdomen, usually the left lower quadrant, due to abnormal rotation of the gut (e.g., situs inversus). lumbar appendicitis. acute appendicitis in a retrodisplaced appendix in the lumbar region. obstructive appendicitis. acute appendicitis due to infection of retained secretion behind an obstruction of the lumen by a fecalith or some other cause, including carcinoma of the cecum. perforating appendicitis. inflammation of the appendix leading to perforation of the wall of the appendix into the peritoneal cavity, resulting in peritonitis. recurrent appendicitis. repeated episodes of right lower quadrant abdominal pain attributed to recurrence of inflammation of the appendix in a person who did not have an appendectomy for prior episodes. SYN: relapsing appendicitis. relapsing appendicitis. SYN: recurrent appendicitis. stercoral appendicitis. appendicitis following a lodgment of fecal material in the appendix. subperitoneal appendicitis. appendicitis of a subperitoneally displaced appendix. suppurative appendicitis. acute appendicitis with purulent exudate in the lumen and wall of the appendix. verminous appendicitis. appendicitis caused by obstruction or in response to the presence of parasitic worms such as Ascaris lumbricoides, Strongyloides stercoralis, or the pinworm Enterobius vermicularis.
and list the most common complications.
Compare and contrast the clinical and pathologic features of