Website Cases:
CASE NUMBER 51
Clinical History: Infectious disease faculty will present the patient.
Summary of Clinical History: A 45-year-old man was brought by his wife to the emergency room with a one-week history of nausea, vomiting and a high fever. His wife stated that he had been confused since he awakened that morning. Further questioning revealed that he had a history of alcoholism and had been on a drinking spree two weeks earlier. Physical exam revealed dry mucus membranes, an elevated heart rate of 120 bpm, and orthostasis.
More detailed examination demonstrated decreased breath sounds and dullness to percussion at the base of the right. Laboratory values were significant for a WBC of 24,000 (60% neutrophils, 24% bands/immature neutrophils, 3% eosinophils, 13% lymphocytes).
The patient was admitted to the hospital for observation, further testing, and treatment. However, while being transferred to the in-patient ward, he experienced cardiorespiratory arrest and could not be resuscitated. Gross and microscopic images from the autopsy are provided.
Path Slide 051:
Image Gallery:
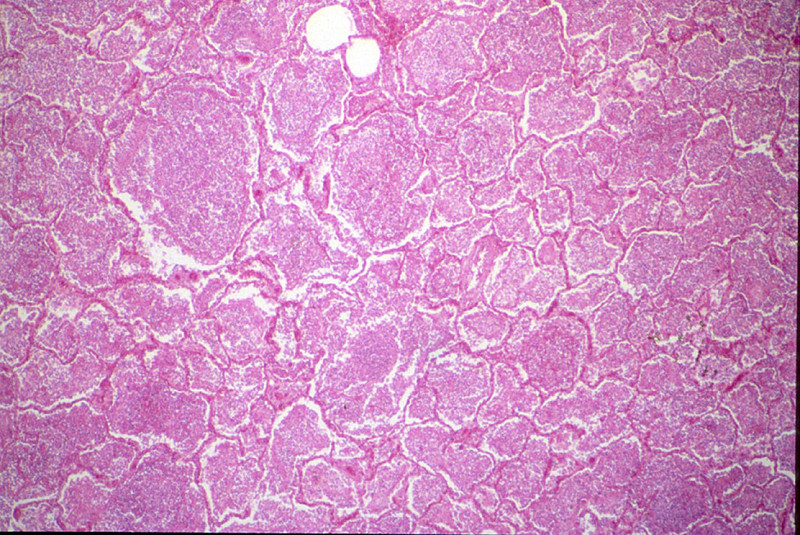
Gram stain of sputum obtained before death shows Gram positive cocci in pairs. The right lung was heavy weighing 700 grams. Its lower lobe showed diffuse gray consolidation. The trachea and bronchi contained a great deal of mucus, and the mucosa was dark red.
|
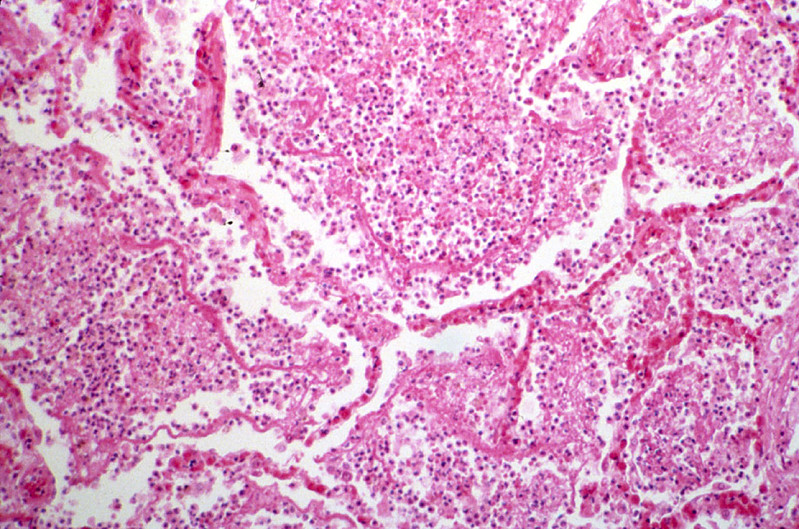
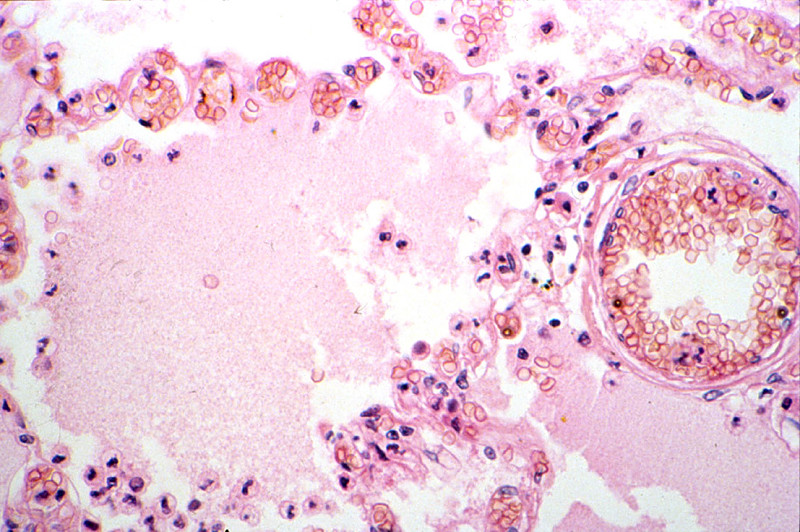
The alveoli are distended and contain a large amount of inflammatory exudate, which consists of many polymorphonuclear leukocytes, a few RBC's, macrophages and strands of fibrin. Many RBC's have been phagocytosed by the macrophages and are undergoing disintegration. The alveolar septa are delicate and well preserved, but markedly congested.
|
(Review Lung Histology)
Norm No. 24 Lung
[ImageScope] [WebScope]
The primary function of the lung is gas exchange. Therefore, alveoli have thin walls lined by thin flat pneumocytes and endothelial cells. There is no thickening or fibrosis of the interstitium. The bronchioli are lined with basally oriented ciliated columnar epithelium. The bronchi are lined by similar epithelium. There are mucous glands within the submucosa. The bronchial smooth muscle is not hypertrophied. The pulmonary vessels are patent with no evidence of intimal thickening or muscular hyperplasia.
|
|
dd
CASE NUMBER 54
[DigitalScope]
[ImageScope] [WebScope]
Clinical History: An 18-year-old woman presented to the Emergency Department with a two-day history of nausea, vomiting and periumbilical and lower abdominal pain. Earlier that day, she experienced shaking chills and fever. Physical exam showed local tenderness and rigidity with rebound pain in the lower abdomen. Laboratory tests revealed a white blood cell count of 21,900/ dL, C-reactive protein of 300 mg/L (normal <3.0 mg/dL) and an erythrocyte sedimentation rate of 104 mm/h (normal 0-20 mm/h). A pregnancy test was negative. A peripheral smear showed immature neutrophils (“band” cells). Abdominal CT showed a dilated appendix with wall thickening and extaluminal fluid.
She underwent an exploratory laparotomy.
Image Gallery:
(Summary of Gross Findings)
The appendix was swollen, dark red, hemorrhagic, and covered by gray-yellow exudate. Serial cross-sections revealed a distended lumen containing hemorrhagic material and a fecalith, which apparently obstructed the lumen.
|
(Summary of Microscopic Findings)
Portions of the mucosa are ulcerated, necrotic and heavily infiltrated with neutrophils. This acute inflammation and necrosis extends throughout the entire thickness of the wall and the serosa. In the lumen of the appendix there is pus and a fecalith. The appendiceal wall is edematous.
|
(Review Normal Histology)
Norm No. 8 Appendix
[ImageScope] [WebScope]
The appendix is a tubular organ with a lumen which is lined by mucin secreting columnar epithelium. Although there are generally numerous lymph nodules in the lamina propria and submucosa under normal conditions, there is no evidence of acute inflammation. The submucosa and muscle layers are unremarkable, and there is no inflammation of the serosa.
|
Gross Image Questions:
- Identify the tip and the lumen of the appendix by annotating a screenshot.
- Describe the appearance of the specimen and how it compares to a typical appendix.
Virtual Microscope Slide Questions:
- Describe what you see on the slide.
- By annotating a screenshot, identify:
- an area of ulcerated mucosa
- a focus of neutrophils
- area of hemorrhage
- an area of relatively unaffected mucosa and,
- the fecalith.
54-1. What is the differential diagnosis?
ANSWER
54-2.Which of the following is the most prominent morphologic pattern of inflammation seen in this case?
- Fibrinous inflammation
- Granulomatous inflammation
- Purulent inflammation
- Serous inflammation
- Ulceration
ANSWER
54-3. Which of the following accounts for the immature neutrophils (“band” cells) seen in the peripheral smear?
- Diapedesis
- Eosinophilia
- Leukopenia
- Mastocytosis
- Shift to the left
ANSWER
54-4. The fever experienced by this patient is MOST LIKELY the result of the formation of which of the following two chemical mediators?
- Complement C3b and IgG
- Interleukin-1 and tumor necrosis factor
- Histamine and serotonin
- Platelet activating factor and bradykinin
- Leukotriene and interleukin-6
ANSWER
54-5. The edematous appearance of the appendix is primarily due to the effects of which of the following inflammatory mediators?
- C3b
- Histamine
- Hydroxyeicosatetraenoic acid (HETE)
- Lipoxin A4
- Thromboxane A2
ANSWER
CASE NUMBER 240
[DigitalScope]
[ImageScope] [WebScope]
Clinical History: A 54-year-old man presented to his primary care physician with a one-year history of intermittent upper abdominal pain. Laboratory results were as follows:
TEST |
RESULT (ref. range in parentheses) |
Hemoglobin |
10 gm/dL (12.0 – 16.0 gm/dL) |
Hct |
37% (41-53%) |
MCV |
61 µm3 (80- 100 µm3) |
MCHC |
28 % Hb/cell (31- 36% Hb/cell) |
Serum ferritin |
2 ng/mL (12-150 ng/mL) |
Upper endoscopy was performed, which revealed a solitary ulcerated lesion. Although most cases of this disease are typically treated medically, this patient underwent a partial gastrectomy.
Image Gallery:
(Summary of Gross Findings)
An endoscopic view shows that the gastric mucosa is somewhat flattened but demonstrates a focal ulcer with smooth edges.
|
(Summary of Microscopic Findings)
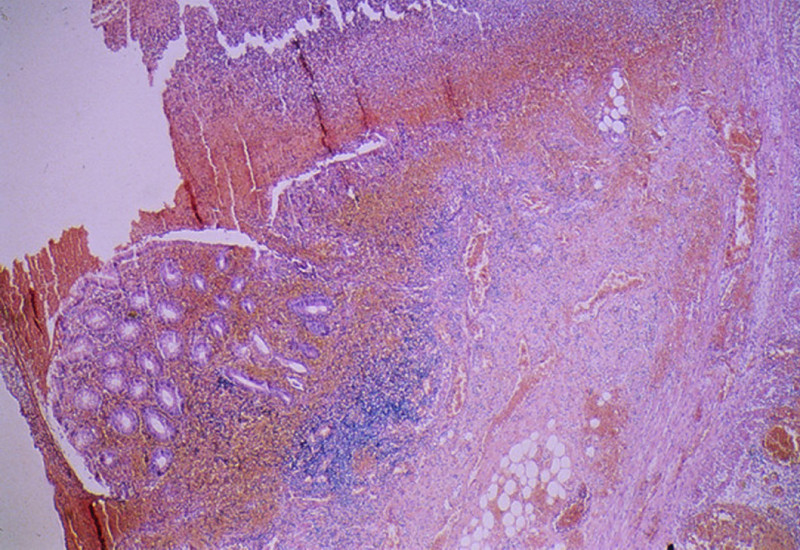
Microscopic sections show a portion of antral/pyloric stomach. A large ulcer and the accompanying response have replaced all layers of the stomach mucosa and wall. Three layers may be distinguished in the bed of the ulcer. The innermost one is composed of necrotic debris and fibrino-purulent exudate in which bacteria and yeast are present. The middle layer is a zone of granulation tissue made up of small vessels and acute and chronic inflammation. The deepest portion of the ulcer is made up of fibrous scar. Some of the arteries in the scar tissue may show sclerosis. The mucosa adjacent to the ulcer shows acute and chronic gastritis. There are lymphoid follicles with germinal centers. In addition, abundant plasma cells are present.
|
(Review Normal Histology)
Norm No. 16 Stomach, fundus
[ImageScope] [WebScope]
The normal gastric mucosa of the fundus contains superficial fovea arranged in leaf like fronds and deeper gastric glands. The foveolar cells secrete mucin. The gastric glands include mucous cells, parietal cells, chief cells and enteroendocrine cells.
|
240-1. What is the differential diagnosis?
ANSWER
240-2. Which of the following cell types is most closely associated with a chronic (as opposed to acute) process?
- Eosinophils
- Neutrophils
- Mast cells
- Monocytes
- Plasma cells
ANSWER
240-3. This specimen shows mixed acute and chronic inflammation. Which of the following best reflects the order of events which led to neutrophil infiltration of the tissue?
- Adhesion, margination, migration through tissues, migration across vessel wall, rolling.
- Adhesion, margination, rolling, migration through tissues, migration across vessel wall.
- Margination, rolling, adhesion, migration across vessel wall, migration through tissues.
- Migration across vessel wall, margination, rolling, adhesion, migration through tissues.
- Rolling, adhesion, margination, migration through tissues, migration across vessel wall.
ANSWER
240-4. Initial rolling interactions are mediated by which of the following?
- Arachidonic acid metabolites
- Cadherins
- Integrins
- Platelet endothelial cell adhesion molecule (PECAM-1)
- Selectins
ANSWER
240-5. In patients with this condition, plain radiographic evidence of free air under the diaphragm in the upright position is most suggestive of which of the following?
- Chronic gastritis
- Frank hemorrhage
- Malignant transformation
- Perforation
- Reactive gastropathy
ANSWER
CASE NUMBER 143
[DigitalScope]
[ImageScope] [WebScope]
Clinical History: A 21-year-old woman presented to her gynecologist with a recently discovered breast mass. Her surgical history was significant for silicone breast augmentation two years earlier. Following ultrasound evaluation, she underwent surgery to remove the breast implant and the associated mass.
Image Gallery:
(Summary of Gross Findings)
The cyst cavity that that surrounded the implant in the body and an example of a commonly used silicone breast implant is shown. The intact implant causes a proliferation of connective tissue that surrounds it. If the implant ruptures or leaks, the silicone causes a foreign body reaction.
|
(Summary of Microscopic Findings)
The irregular fragments of foreign material are surrounded or engulfed by multinucleated foreign body giant cells. The rest of the section is made up of fibrous connective tissue and collections of lymphocytes and histiocytes (macrophages).
|
(Review Normal Histology)
Norm No. 19 Female breast
[ImageScope] [WebScope]
The female breast is a secretory organ that produces milk during lactation. Breast tissue that is not stimulated to lactate consists of resting apocrine cells arranged in nests and small ductules which are lined by cuboidal epithelium. The secretory units are separated from one another by loose connective tissue.
|
|
143-1. What is the differential diagnosis?
ANSWER
143-2. Which of the following processes is represented in these microscopic images?
- Acute inflammation
- Amyloidosis
- Caseous necrosis
- Chronic inflammation
- Granulomatous inflammation
ANSWER
143-3. Which type of cell aggregates to form the multinucleated giant cells seen here?
- Basophils
- Eosinophils
- Macrophages
- Neutrophils
- Plasma cells
ANSWER
143-4. Microscopically, there is dense fibrosis. Which of the following stimulates the production of collagens and fibronectin in this clinical setting?
- Matrix metalloproteinase
- Nitric oxide
- Transforming growth factor (TGF)-beta
- Tumor necrosis factor (TNF)
- Vascular endothelial growth factor (VEGF)
ANSWER
INFLAMMATION Review Items
Key Vocabulary Terms (click here to search any additional terms on Stedman's Online Medical Dictionary)
INFLAMMATION GOALS and LEARNING OBJECTIVES:
Goal 1: Mechanisms of Inflammation
Apply knowledge of the biochemistry and cellular physiology to describe pathogenic mechanisms of acute and chronic inflammation, and the resulting pathology at the cellular, tissue, and organism levels.
- Objective 1: Acute Inflammatory Response
Describe the time course of the vascular and cellular events responsible for the acute inflammatory response to injury, and discuss the receptors and ligands that are responsible for these events.
- Objective 2: Phagocytosis
Describe phagocytosis and the molecular mechanisms of intracellular killing.
- Objective 3: Mediators of Inflammation
Discuss the chemical mediators of inflammation, classifying the mediators with respect to origins, targets, and mechanisms of action.
- Objective 4: Systemic Changes in Inflammation
Describe systemic changes seen in inflammation, including metabolic consequences of changes in levels of serum proteins (acute phase reactants) and other inflammatory mediators.
- Objective 5: Outcomes of Inflammation
Summarize the possible pathological outcomes of inflammation and discuss factors that determine what outcomes are seen under different circumstances.
- Objective 6: Morphologic Patterns of Inflammation
Recognize and classify the major types of inflammatory lesions that can be present in histologic sections, and identify the cellular constituents in these lesions.
- Objective 7: Acute, Chronic, and Granulomatous Inflammation
Compare and contrast acute, chronic, and granulomatous inflammation with respect to the major cell type(s) involved in the processes, the types of etiologic agents that produce each of these, and the mechanisms of tissue injury seen with these different types of inflammation.
- Objective 8: Extravascular Fluids Associated With Injury
Classify types of extravascular fluids associated with injury based on their cellular and protein content, know the terminology used to define these, and provide examples of pathologic conditions in which these can be found.
Goal 2: Mechanisms of Tissue Regeneration, Renewal and Repair
Apply knowledge of biochemistry and cellular physiology to describe the pathogenic mechanisms of tissue regeneration, renewal and repair, the resulting pathology at the cellular, tissue and organism levels, and describe clinical manifestations.
- Objective 1: Stem Cells
Compare and contrast embryonic and adult (somatic) stem cells with respect to their ability to proliferate and differentiate into different cell types; define induced pluripotent stem cells and compare and contrast them with the other types of stem cells.
- Objective 2: Extracellular Matrix
List the important proteins of the extracellular matrix, describe the importance of cell-matrix interactions in the regulation of cell growth and differentiation, and provide examples of how structural alterations of matrix proteins produce disease.
- Objective 3: Angiogenesis
Describe the regulation of angiogenesis, discussing receptors on vascular endothelium as well as the role soluble and stromal factors play in the process.
- Objective 4: Wound Healing
Describe the phases of cutaneous wound healing and the mechanisms of healing by first intention (primary union) and second intention (secondary union).
Click here to submit questions or comments about this site.
Duke University | Duke Medicine | School of Medicine | School of Nursing | Doctor of Physical Therapy
Copyright © 2004-2021 Duke University School of Medicine
Updated 12/30/20 - Velkey |

















{kind=link}