Case assignments by lab group and class day
| |
WEDNESDAY |
THURSDAY |
| Labs 1, 2, & 3 |
|
|
| |
|
|
| Labs 4, 5, & 6 |
|
|
| |
|
|
CASE NUMBER 31
[ImageScope] [WebScope]
Clinical History: A 55-year-old man with history of uncontrolled diabetes and hypertension presented to the emergency department with a 3-day history of nagging chest pain. Four hours earlier, the chest pain got much worse and radiated to both arms and his neck. It was accompanied by diaphoresis and dyspnea.
On exam: BP 160/100, HR 110, RR 24, O2 98% on room air. Heart rate is regular and there is trace bilateral edema. CBC and BMP are unremarkable. CK-MB is 42, CK 300, Troponin T 0.89. ECG shows 3 mm of ST elevation in leads V2-V4.
The cardiac catherization lab treats him with thrombolytic agents for a diagnosis of ST elevation myocardial infarction. Approximately 20 minutes after infusion begins, he experiences ventricular tachycardia and dies.
Image Gallery:
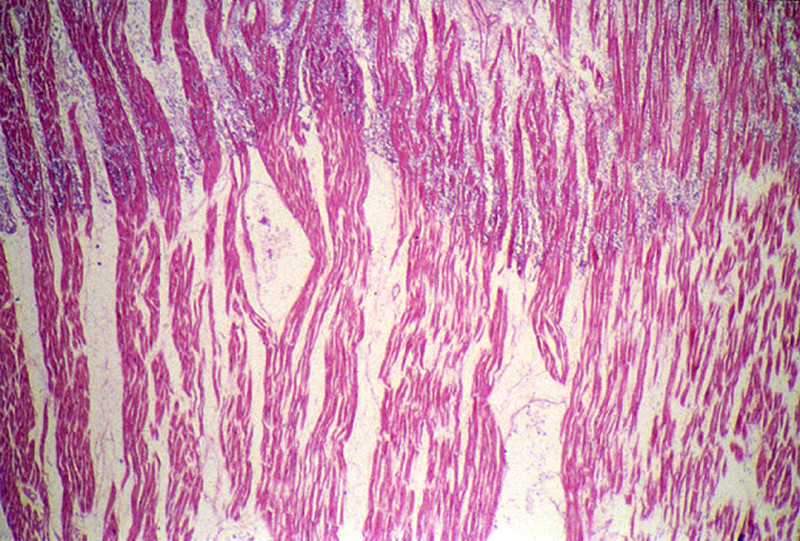
The heart was slightly enlarged weighing 460gms. There was severe atherosclerosis of all the major coronary arteries with a recent thrombotic occlusion of the proximal left anterior descending coronary artery. A recent transmural infarct was present in the left ventricle that involved the interventricular septum and the papillary muscle.
|
The slide includes a transmural section of the left ventricle. Nearly the entire section is involved by infarct. However, there is a thin rim (5 to 10 cell layers) of endocardial myocytes which have survived because of diffusion of oxygen and nutrients from the ventricular cavity. Other viable myocytes can be found around larger blood vessels within the section. The intense hypereosinophilia of the necrotic myocytes can best be appreciated by comparing the thin rim of lighter staining subendocardial myocytes with the deeper cells. Note also the karyolysis that is characteristic of coagulation necrosis. In some areas there is little inflammatory response. This observation is explained by microvascular necrosis which does not allow access of circulating leukocytes to these areas. In other areas, especially in the epicardial half of the infarct, there is an intense acute inflammatory response. Many intact neutrophils can be seen. In addition, there are many nuclear fragments from lysed neutrophils. Macrophage activity is not evident. These features of the inflammatory response indicate that the infarct was approximately three to four days old. Note also that the inflammation extends to the epicardial surface and that there are deposits of fibrin on the epicardium. This is called fibrinous pericarditis. The granular grey material seen within some blood vessels is barium sulfate, which was injected to permit post-mortem study of the coronaries by radiography.
|
(Review Normal Histology)
Norm No. 13 Heart
[ImageScope] [WebScope]
Normal heart tissue sections demonstrate no evidence of fibrosis or hemorrhage. Cardiac myocytes have moderately sized centrally located nuclei. Normal myocytes are not brightly eosinphilic. Normally no inflammation is seen. Normal cardiac myocytes do not show hypertrophy.
|
31-1. Which of the following best describes the pathologic findings?
- Caseous necrosis
- Coagulative necrosis
- Fat necrosis
- Fibrinoid necrosis
- Gangrenous necrosis
31-2. Which of the following best describes the nuclear changes seen here?
- Chromatin condensation
- DNA cleavage into nucleosomal subunits
- Karyorrhexis
- Karyolysis
- Pyknosis
31-3. Increased eosinophilia of the dead myocytes is most directly linked to which of the following molecular events?
- Cytoplasmic blebbling
- Denaturation of cytoplasmic proteins
- Increased cytoplasmic RNA
- Generation of myelin figures
- Loss of glycogen particles
31-4. Which of the following is a feature of necrosis?
- Caspase activation
- Chromatin condensation
- Cytoplasmic blebbing
- DNA cleavage into nucleosomal subunits
- Karyorrhexis
31-5. Which of the following is the most likely explanation for the onset of ventricular tachycardia following initiation of thrombolytic therapy?
- Direct toxic effect of the thrombolytic therapy
- Reperfusion injury
- Second thrombus in the same site
- Systemic hypotension
- Ventricular rupture
CASE NUMBER 370 - slide courtesy of UMich
[ImageScope] [WebScope]
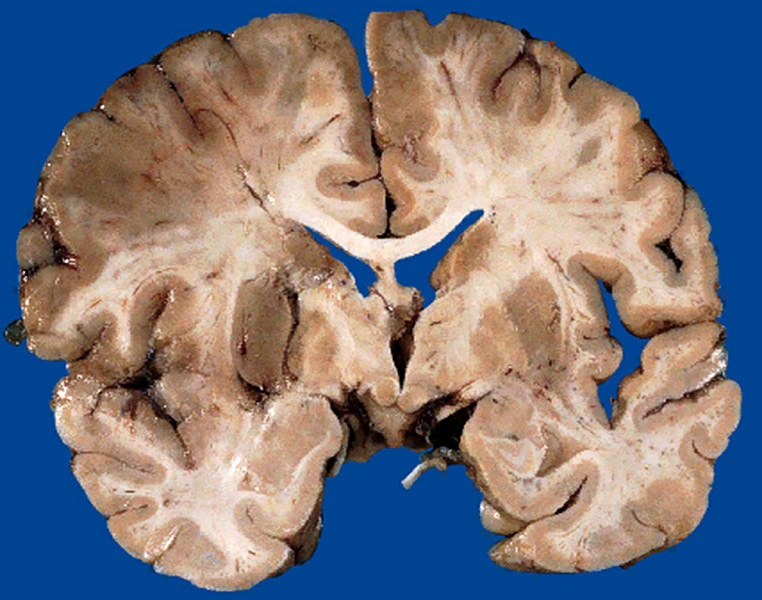
Clinical History: A 67-year-old woman with a long history of hypertension and a remote myocardial infarction presented to the emergency department with a two-hour history of left-sided weakness. She reported that she had a “fluttering” sensation in her chest and that her cardiologist had recommended treatment for atrial fibrillation which she had refused. While in the emergency department, she developed left-sided hemiparesis. She was admitted to the hospital for observation; however, her condition worsened and she went into a coma. She died 17 days after admission.
Image Gallery:
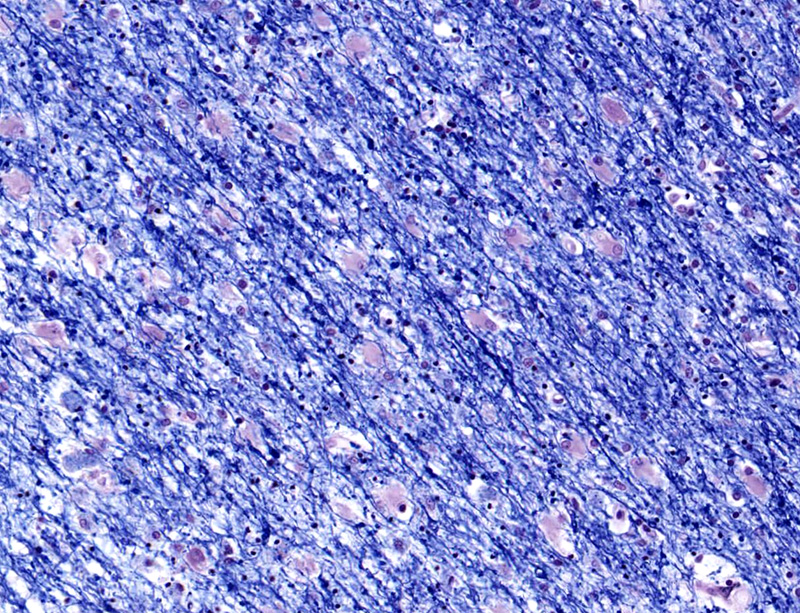
There was thrombosis of the right internal carotid artery just above the bifurcation. There was extensive necrosis of the right frontal, parietal and temporal lobes and basal ganglia.
|
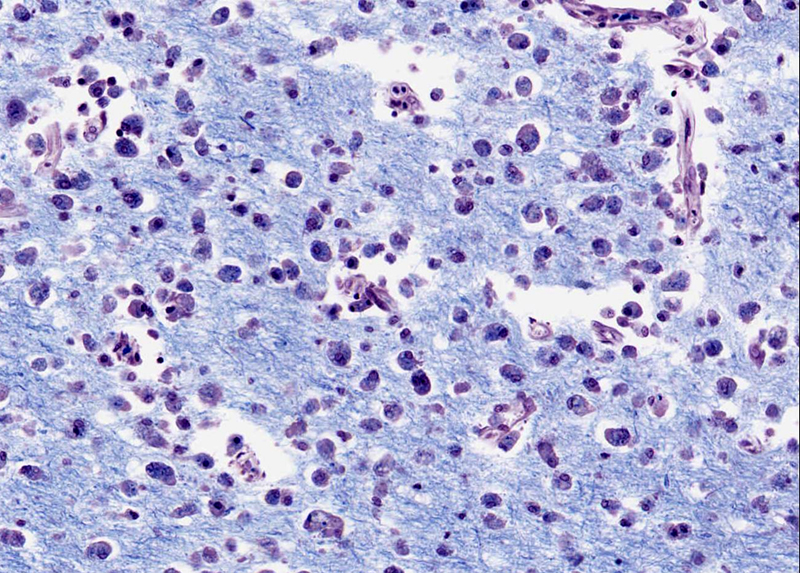
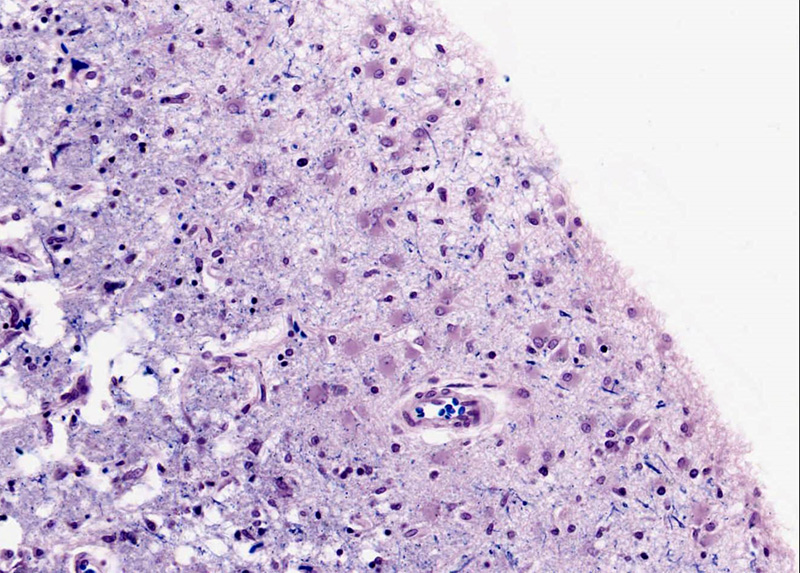
This is a luxol stain, which stains cell bodies (most abundant in the cortex) light pink whereas myelin (most abundant in the white matter) is dark blue. There is an area of liquefactive necrosis in which many macrophages with phagocytosed fat and myelin particles are present. At the pial surface and within the white matter surrounding the necrotic area are numerous large astrocytes (reactive gliosis) with large vesicular nuclei and abundant eosinophilic cytoplasm. The myelin in this area stains pale (compared to more healthy white matter seen on the right side of the slide) due to surrounding edema fluid. The blood vessels are congested and there is some extravasated blood.
|
(Review Normal Histology)
Norm No. 16 Stomach, fundus
[ImageScope] [WebScope]
The normal gastric mucosa of the fundus contains superficial fovea arranged in leaf like fronds and deeper gastric glands. The foveolar cells secrete mucin. The gastric glands include mucous cells, parietal cells, chief cells and enteroendocrine cells.
|
370-1. Which of the following best describes the pathologic findings?
- Caseous necrosis
- Coagulative necrosis
- Fat necrosis
- Liquefactive necrosis
- Gangrenous necrosis
370-2. Which of the following processes did the necrotic cells in this specimen undergo?
- Caspase activation
- Cell shrinkage
- Chromatin condensation
- DNA cleavage into nucleosomal subunits
- Loss of membrane integrity
370-3. When the patient’s artery was initially occluded by thrombus, ischemia led to a rapid decrease in intracellular ATP levels. Which of the following is a consequence of this process?
- Efflux of calcium
- Detachment of ribosomes
- Increased pH
- Influx of potassium
- Decrease in anaerobic glycolysis
370-4. In this ischemic environment, the mitochondria are unable to maintain normal oxidative phosphorylation, resulting in release of reactive oxygen species into the cytoplasm. Which of the following is the most direct consequence of this release?
- Apoptosis
- Failure of the Ca2+ pump
- Increased phospholipid breakdown
- Leakage of metabolites into the extracellular space
- Lipid peroxidation of membranes
CASE NUMBER 85:
[ImageScope] [WebScope]
Clinical History: A 64-year-old morbidly obese woman was admitted to the emergency department with a 6-hour history of nausea, vomiting and jaw pain. While she was in the emergency department she collapsed and died. Autopsy revealed a massive myocardial infarction as well as significant liver pathology.
Image Gallery:
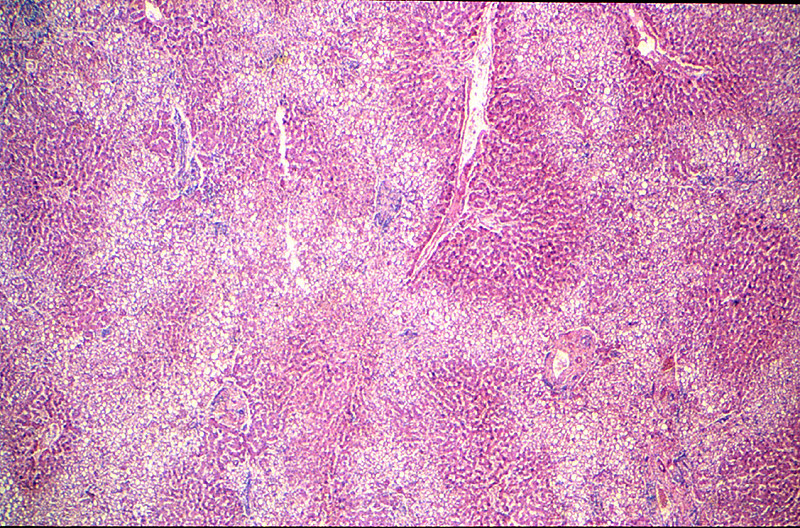
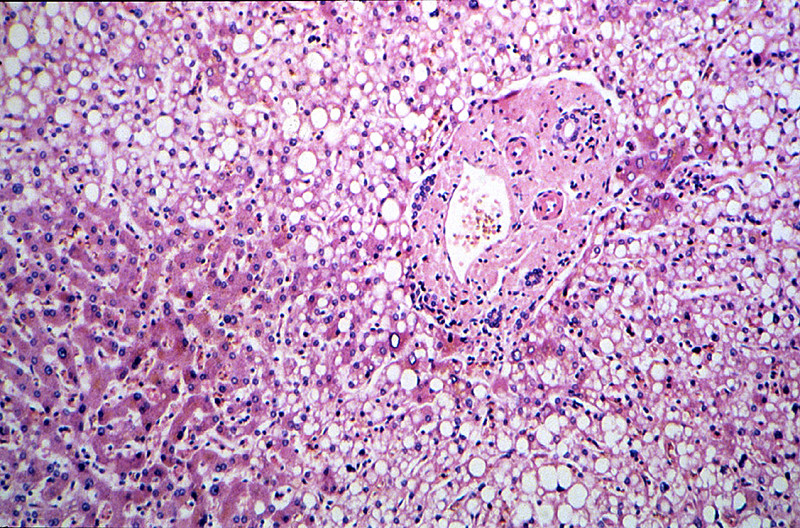
The liver weighed 1980 grams. It had a pale, greasy appearance.
|
The areas of fatty change are readily visible with use of scanning power. They are zonal. Note the peri-portal areas are severely involved and the areas of fatty change extend from one portal area to another. The more severely involved cells have eccentric nuclei and the entire cytoplasm is replaced by a fat globule.
|
(Review Normal Histology)
Norm No. 3 Liver
[ImageScope] [WebScope]
The liver is the organ that metabolizes nutrients received from the digestive tract. These nutrients and processed by tissue hepatocytes which are large polygonal cells. The hepatocyes are separated by portal triads. The triads consist of an artery, a vein and a bile duct. The bile duct is lined by cuboidal epithelium. The artery has a muscular wall and a flat endothelial lining. The sinuses are well defined and contain a small amount of blood.
|
240-1. What is the differential diagnosis?
240-2. Which of the following cell types is most closely associated with a chronic (as opposed to acute) process?
- Eosinophils
- Neutrophils
- Mast cells
- Monocytes
- Plasma cells
240-3. This specimen shows mixed acute and chronic inflammation. Which of the following best reflects the order of events which led to neutrophil infiltration of the tissue?
- Adhesion, margination, migration through tissues, migration across vessel wall, rolling.
- Adhesion, margination, rolling, migration through tissues, migration across vessel wall.
- Margination, rolling, adhesion, migration across vessel wall, migration through tissues.
- Migration across vessel wall, margination, rolling, adhesion, migration through tissues.
- Rolling, adhesion, margination, migration through tissues, migration across vessel wall.
240-4. Initial rolling interactions are mediated by which of the following?
- Arachidonic acid metabolites
- Cadherins
- Integrins
- Platelet endothelial cell adhesion molecule (PECAM-1)
- Selectins
240-5. In patients with this condition, plain radiographic evidence of free air under the diaphragm in the upright position is most suggestive of which of the following?
- Chronic gastritis
- Frank hemorrhage
- Malignant transformation
- Perforation
- Reactive gastropathy
CASE NUMBER 143
[ImageScope] [WebScope]
Clinical History: A 21-year-old woman presented to her gynecologist with a recently discovered breast mass. Her surgical history was significant for silicon breast augmentation two years earlier. Following ultrasound evaluation, she underwent surgery to remove the breast implant and the associated mass.
Image Gallery:
The cyst cavity that that surrounded the implant in the body and an example of a commonly used silicone breast implant is shown. The intact implant causes a proliferation of connective tissue that surrounds it. If the implant ruptures or leaks, the silicone causes a foreign body reaction.
|
The irregular fragments of foreign material are surrounded or engulfed by multinucleated foreign body giant cells. The rest of the section is made up of fibrous connective tissue and collections of lymphocytes and histiocytes (macrophages).
|
(Review Normal Histology)
Norm No. 19 Female breast
[ImageScope] [WebScope]
The female breast is a secretory organ that produces milk during lactation. Breast tissue that is not stimulated to lactate consists of resting apocrine cells arranged in nests and small ductules which are lined by cuboidal epithelium. The secretory units are separated from one another by loose connective tissue.
|
|
143-1. What is the differential diagnosis?
143-2. Which of the following processes is represented in these microscopic images?
- Acute inflammation
- Amyloidosis
- Caseous necrosis
- Chronic inflammation
- Granulomatous inflammation
143-3. Which type of cell aggregates to form the multinucleated giant cells seen here?
- Basophils
- Eosinophils
- Macrophages
- Neutrophils
- Plasma cells
143-4. Microscopically, there is dense fibrosis. Which of the following stimulates the production of collagens and fibronectin in this clinical setting?
- Matrix metalloproteinase
- Nitric oxide
- Transforming growth factor (TGF)-beta
- Tumor necrosis factor (TNF)
- Vascular endothelial growth factor (VEGF)
INFLAMMATION Review Items
Key Vocabulary Terms (click here to search any additional terms on Stedman's Online Medical Dictionary)
INFLAMMATION GOALS and LEARNING OBJECTIVES:
Goal 1: Mechanisms of Inflammation
Apply knowledge of the biochemistry and cellular physiology to describe pathogenic mechanisms of acute and chronic inflammation, and the resulting pathology at the cellular, tissue, and organism levels.
- Objective 1: Acute Inflammatory Response
Describe the time course of the vascular and cellular events responsible for the acute inflammatory response to injury, and discuss the receptors and ligands that are responsible for these events.
- Objective 2: Phagocytosis
Describe phagocytosis and the molecular mechanisms of intracellular killing.
- Objective 3: Mediators of Inflammation
Discuss the chemical mediators of inflammation, classifying the mediators with respect to origins, targets, and mechanisms of action.
- Objective 4: Systemic Changes in Inflammation
Describe systemic changes seen in inflammation, including metabolic consequences of changes in levels of serum proteins (acute phase reactants) and other inflammatory mediators.
- Objective 5: Outcomes of Inflammation
Summarize the possible pathological outcomes of inflammation and discuss factors that determine what outcomes are seen under different circumstances.
- Objective 6: Morphologic Patterns of Inflammation
Recognize and classify the major types of inflammatory lesions that can be present in histologic sections, and identify the cellular constituents in these lesions.
- Objective 7: Acute, Chronic, and Granulomatous Inflammation
Compare and contrast acute, chronic, and granulomatous inflammation with respect to the major cell type(s) involved in the processes, the types of etiologic agents that produce each of these, and the mechanisms of tissue injury seen with these different types of inflammation.
- Objective 8: Extravascular Fluids Associated With Injury
Classify types of extravascular fluids associated with injury based on their cellular and protein content, know the terminology used to define these, and provide examples of pathologic conditions in which these can be found.
Goal 2: Mechanisms of Tissue Regeneration, Renewal and Repair
Apply knowledge of biochemistry and cellular physiology to describe the pathogenic mechanisms of tissue regeneration, renewal and repair, the resulting pathology at the cellular, tissue and organism levels, and describe clinical manifestations.
- Objective 1: Stem Cells
Compare and contrast embryonic and adult (somatic) stem cells with respect to their ability to proliferate and differentiate into different cell types; define induced pluripotent stem cells and compare and contrast them with the other types of stem cells.
- Objective 2: Extracellular Matrix
List the important proteins of the extracellular matrix, describe the importance of cell-matrix interactions in the regulation of cell growth and differentiation, and provide examples of how structural alterations of matrix proteins produce disease.
- Objective 3: Angiogenesis
Describe the regulation of angiogenesis, discussing receptors on vascular endothelium as well as the role soluble and stromal factors play in the process.
- Objective 4: Wound Healing
Describe the phases of cutaneous wound healing and the mechanisms of healing by first intention (primary union) and second intention (secondary union).
Click here to submit questions or comments about this site.
Duke University | Duke Medicine | School of Medicine | School of Nursing | Doctor of Physical Therapy
Copyright © 2004-2019 Duke University School of Medicine
Updated 1/30/19 - Velkey |