CASE NUMBER 158
[ImageScope] [WebScope]
Clinical History: A 63-year-old man presented to the emergency department with a two-day history of severe chest pain and dyspnea. Past medical history was relevant for a 5-year history of congestive heart failure and progressive weakness. While he was in the emergency department, he collapsed and died.
Image Gallery:
(Summary of Gross and Lab Findings - click here)
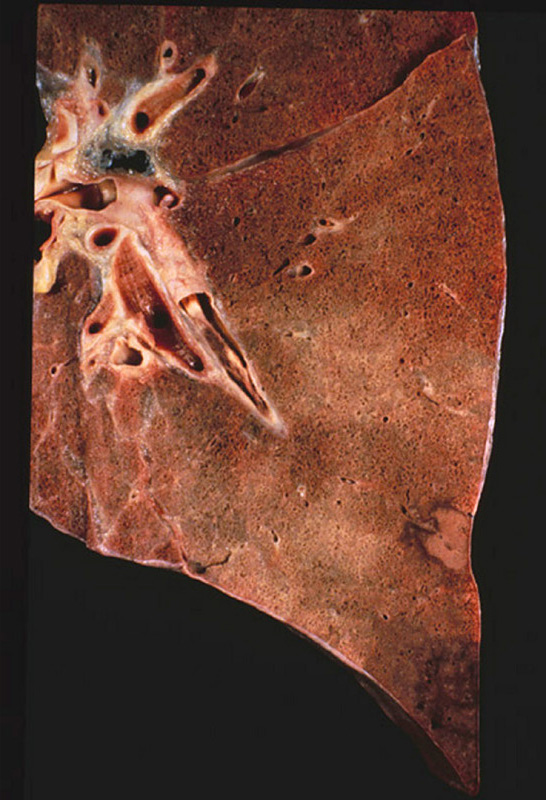
The lung was dark red and heavy, and a large amount of hemorrhagic frothy fluid exuded freely from the cut surface. In the main pulmonary artery there was a large red firm clot adherent to the vascular wall. Many small blood clots were present in the vessels of the upper and lower lobes. Associated with these were many wedge-shaped, dark red, firmer areas in the lung parenchyma.
|
(Summary of Microscopic Findings - click here)
There are two sections on the slide. On one section there are organizing thrombi in the pulmonary arteries. On the other section there is a large hemorrhagic area in which some alveolar septa are pink, smudgy, and necrotic. In other portions of the lung the septa are thickened with fibrosis..
|
(Review Normal Histology - click here)
Norm No. 24 Lung
[ImageScope] [WebScope]
The primary function of the lung is gas exchange. Therefore, alveoli have thin walls lined by thin flat pneumocytes and endothelial cells. There is no thickening or fibrosis of the interstitium. The bronchioli are lined with basally oriented ciliated columnar epithelium. The bronchi are lined by similar epithelium. There are mucous glands within the submucosa. The bronchial smooth muscle is not hypertrophied. The pulmonary vessels are patent with no evidence of intimal thickening or muscular hyperplasia.
|
158-1. What is the differential diagnosis?
ANSWER
158-2. In cases of deep venous thrombosis with embolism, which vessels are most often occluded?
- Bronchial arteries
- Bronchial veins
- Inferior vena cava
- Pulmonary arteries
- Pulmonary veins
- Superior vena cava
ANSWER
158-3. Pulmonary emboli are more common than pulmonary infarcts. Which of the following explains this observation?
- Coagulation is slower in oxygenated tissue
- Lung tissue has increased numbers of mitochondria
- Lungs have a dual arterial supply
- Oxygenation can occur across the bronchial wall
- Venous drainage is accelerated in lung tissue
ANSWER
158-4. What do the firm, red, wedge-shaped areas of the lung represent?
- Angiosarcoma
- Hemorrhage
- Infarcts
- Metastatic disease
- Thrombosis
ANSWER
CASE NUMBER 370 - slide courtesy of UMich
[ImageScope] [WebScope]
Clinical History: A 67-year-old woman with a long history of hypertension and a remote myocardial infarction presented to the emergency department with a two-hour history of left-sided weakness. She reported that she had a “fluttering” sensation in her chest and that her cardiologist had recommended treatment for atrial fibrillation which she had refused. While in the emergency department, she developed left-sided hemiparesis. She was admitted to the hospital for observation; however, her condition worsened and she went into a coma. She died 17 days after admission.
Image Gallery:
(Summary of Gross Findings - click here)
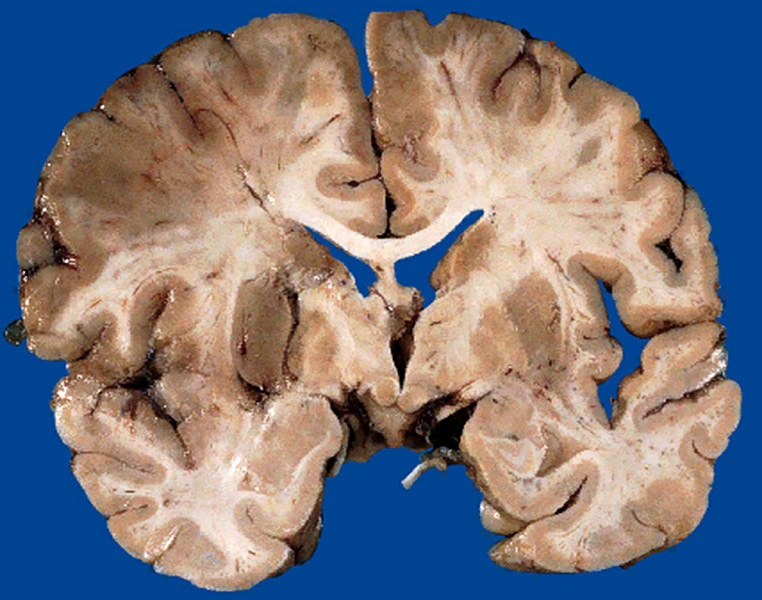
There is a recent infarct in the right middle cerebral artery territory which involved the primary motor cortex as well as the lenticulostriate arteries serving the putamen, caudate, and internal capsule.
|
(Summary of Microscopic Findings - click here)
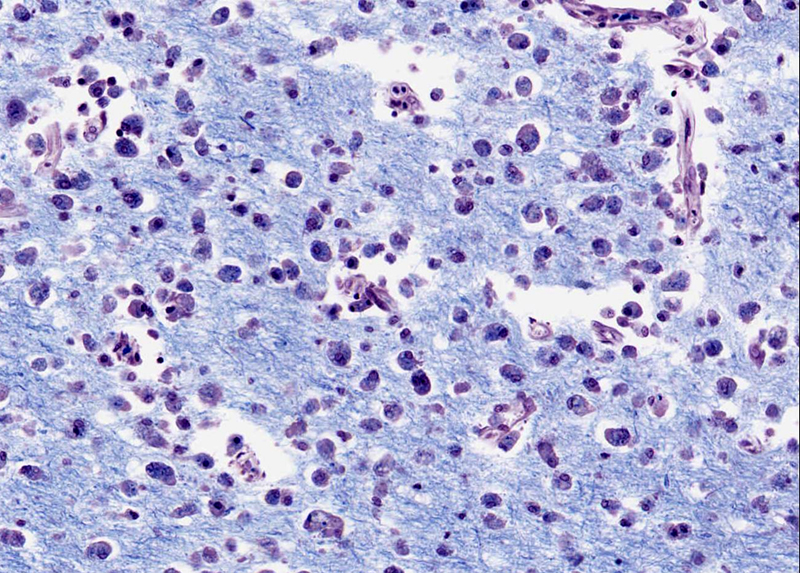
There is an area of liquefactive necrosis in the infarcted cerebral cortex. The myelin in this area stains pale due to surrounding edema fluid. The blood vessels are congested and there is some extravasated blood. (Luxol blue stain)
|
(Review Normal Histology - click here)
Cerebrum
Slide 76 (cerebrum, luxol blue/cresyl violet) [WebScope] [ImageScope]
Slide 76b (toluidine blue & eosin) [WebScope] [ImageScope]
The cerebral cortex is loosely stratified into layers containing scattered nuclei of both neurons and glial cells. Examine the layered organization of the cerebral cortex using slide 76 stained with luxol blue/cresyl violet [ORIENTATION] (which stains white matter tracts and cell bodies) or toluidine blue and eosin [ORIENTATION] (TB&E, toluidine blue stains the nuclei and RER of cells whereas eosin stains membranes and axon tracts). Typically one or more sulci (infoldings) will extend inward from one edge of the section. Examine the gray matter on each side of the sulcus using first low and then high power. Neurons of the cerebral cortex are of varying shapes and sizes, but the most obvious are pyramidal cells. As the name implies, the cell body is shaped somewhat like a pyramid, with a large, branching dendrite extending from the apex of the pyramid toward the cortical surface, and with an axon extending downward from the base of the pyramid. In addition to pyramidal cells, other nuclei seen in these sections may belong to other neurons or to glial cells also present in the cortex. You may be able to see subtle differences in the distribution of cell types in rather loosely demarcated layers. There are 6 classically recognized layers of the cortex:
- Outer plexiform (molecular) layer: sparse neurons and glia
- Outer granular layer: small pyramidal and stellate neurons
- Outer pyramidal layer: moderate sized pyramidal neurons (should be able to see these in either luxol blue [example] or TB&E-stained [example] sections)
- Inner granular layer: densely packed stellate neurons (usually the numerous processes aren’t visible, but there are lots of nuclei reflecting the cell density)
- Ganglionic or inner pyramidal layer: large pyramidal neurons (should be able to see these in either luxol blue [example] or TB&E-stained [example] sections)
- Multiform cell layer: mixture of small pyramidal and stellate neurons
Pyramidal cells in layers III and V tend to be larger because their axons contribute to efferent projections that extend to other regions of the CNS –pyramidal neurons in layer V of motor cortices send projections all the way down to motor neurons in the spinal cord!
Deep to the gray matter of the cerebral cortex is the white matter that conveys myelinated fibers between different parts of the cortex and other regions of the CNS. Be sure you identify the white matter in both luxol blue [example] and TB&E-stained [example] sections, as it will appear differently in these two stains. Review the organization of gray and white matter in cerebral cortex vs. spinal cord.
|
|
370-1. What is the differential diagnosis?
ANSWER
370-2. Which of the following is the most likely etiology of her condition?
- Direct parenchymal injury
- Hypotension
- Infectious vasculitis
- Thromboembolism
- Traumatic vascular injury
ANSWER
370-3. Which of the following are the enlarged foamy cells seen in the high power histologic image?
- Lymphocytes
- Macrophages
- Neurons
- Neutrophils
ANSWER
CASE NUMBER 514
(no virtual slides for this case)
Clinical History: A 28-year-old Caucasian woman presents to the Emergency Department with an acute onset of severe dyspnea after disembarking from a trans-Atlantic flight. She reports left-sided chest pain on inspiration. She has no significant medical history, but states that she takes oral contraceptive pills. Physical exam shows 20 breaths per minute and a heart rate of 125 bpm. Her left calf is swollen and warm. A duplex ultrasound demonstrates a deep venous thrombosis. Laboratory analysis reveals a positive activated protein C resistance test; remaining studies are noncontributory.
Image Gallery:
514-1. Which of the following is the most likely etiology for her condition?
- Antiphospholipid antibody syndrome
- Factor V Leiden mutation
- Glucose-6-phosphate dehydrogenase deficiency
- Hyperhomocystenemia
- von Willebrand disease
ANSWER
514-2. Which of the following is true about this disease?
- Homozygotes have a 50-fold increase in relative risk of venous thrombosis
- Inheritance is typically autosomal recessive
- It is associated with increased prothrombin levels
- Partial thromboplastin time is typically prolonged
- There is an increased incidence in patients with systemic lupus erythematosus
ANSWER
514-3. Which of the following is the pathophysiology of this disease?
- Autoantibodies cause platelet aggregation
- Factor V is resistant to cleavage
- Prothrombin is resistant to cleavage
- Thioester linkages form between homocysteine metabolites and proteins
- Ultra large von Willebrand multimers are found in the serum
ANSWER
514-4. Genetic analysis would most likely show which of the following?
- A chromosomal translocation
- A missense mutation
- A nonsense mutation
- A partial deletion of chromosome 12
- Ring chromosomes
ANSWER
Review Items
THROMBOSIS, HEMOSTASIS, EDEMA, and SHOCK
Key Vocabulary Terms
HEMOSTASIS and THROMBOSIS LEARNING OBJECTIVES
Absolutely critical information you must know to practice medicine is in bold font.
Important information that will be needed for routine patient care is in regular font.
Information about less common diseases that you may encounter in clinical practice and that will probably appear on examinations is in italics.
- Outline the process of normal hemostasis; role and interaction of each element
- Intrinsic pathway
- extrinsic pathway
- final common pathway
- fibrin formation and fibrinolysis
- protein C/protein S pathway
- role of platelets
- role of vascular integrity
- events in dissolution of a thrombus
- Compare acute and chronic hemorrhage in terms of:
- common causes
- clinical manifestations
- compensatory mechanisms
- Describe thrombi in terms of:
- types of thrombotic material
- factors conditioning the development of thrombi
- possible fate of thrombi
- Distinguish between venous thrombi and arterial thrombi on the basis of:
- etiologic and precipitating factors
- common sites of occurrence
- type and size of vessel involved
- morphologic appearance
- organs commonly involved
- local and distant effects
- fate of lesions and prognosis
- clinical and laboratory features
- Compare the following types of emboli in terms of morphologic features, precipitating factors, common sites, organs involved, type of vessel, complications, clinical presentation
- Compare and contrast arterial and venous infarcts on the basis of:
- location
- pathogenesis
- morphology
- clinical manifestations
- Describe the morphologic appearance and natural history of infarcts of:
- heart
- lung
- bowel
- kidney
- spleen
- brain
- Define, state the significance of, and identify on a peripheral blood smear:
- Discuss thrombocytopoiesis in terms of:
- morphology of megakaryocytes
- fate of megakaryocytes
- life span of platelets
- factors which influence thrombocytopoiesis
- abnormal morphologic forms of platelets and megakaryocytes
- Discuss thrombocytopenia in terms of:
- differential diagnosis
- clinical features
- bone marrow morphology and
- laboratory features
- Compare and contrast bleeding due to:
- vascular defect (localized or generalized)
- platelet defect
- coagulation defect
- Discuss thrombocytosis in terms of diagnosis and differential diagnosis
- Outline the process for stepwise evaluation of a:
- bleeding patient
- patient with suspected platelet disorder
- patient with suspected hypercoagulability
- Compare and contrast:
- List and discuss the laboratory diagnostic procedures for patients with:
- bleeding disorders
- thrombotic disorders
- Compare and contrast bleeding disorders due to:
- Describe the mechanism(s) by which the following drugs affect hemostasis:
- aspirin
- coumadin (warfarin)
- heparin
EDEMA AND SHOCK LEARNING OBJECTIVES
Absolutely critical information you must know to practice medicine is in bold font.
Important information that will be needed for routine patient care is in regular font.
Information about less common diseases that you may encounter in clinical practice and that will probably appear on examinations is in italics.
- Compare and contrast the following types of shock:
- List the morphologic changes and functional effects of shock on:
- lungs
- kidneys
- adrenals
- brain
- gastrointestinal tract
- Compare and contrast
- Compare:
- Describe chronic passive congestion in:
- lung
- liver
- kidneys
- spleen
- Discuss the pathogenesis of edema, giving examples associated with:
- altered plasma oncotic pressure
- inflammation
- venous obstruction/stasis
- lymphatic obstruction
- Compare the consequences of edema in:
- subcutaneous tissue
- lungs
- brain
- kidneys
HEMODYNAMICS AND ARTERIOSCLEROSIS
Key Vocabulary Terms
HEMODYNAMICS and ARTERIOSCLEROSIS LEARNING OBJECTIVES
Absolutely critical information you must know to practice medicine is in bold font.
Important information that will be needed for routine patient care is in regular font.
Information about less common diseases that you may encounter in clinical practice and that will probably appear on examinations is in italics.
- Discuss mechanisms of blood pressure regulation, including:
- cardiac influences
- neural factors
- hormonal factors
- vasoactive agents
- renin-angiotensin system
- Compare and contrast clinical and pathologic features of the following types of hypertension:
- Discuss the morphologic effects of hypertension on:
- heart
- brain
- kidneys
- placenta
- Discuss the clinical and pathologic features of the following vascular diseases :
- Discuss the clinical and pathologic features of the following forms of vasculitis:
- Compare and contrast the clinical and pathologic features of the following disorders:
- Compare and contrast thoracic and abdominal aortic aneurysms on the basis of:
- etiologic factors
- incidence
- complications
- Discuss the effects of the following on the pathogenesis and prevalence of atherosclerosis:
- age
- sex
- geographic location
- risk factors
- Outline the development of the atherosclerotic lesion with respect to:
- pathogenic mechanisms
- morphology
- clinical manifestations
- complications
- Compare and contrast the clinical and pathologic features of:
|