CASE NUMBER 220
[ImageScope] [WebScope]
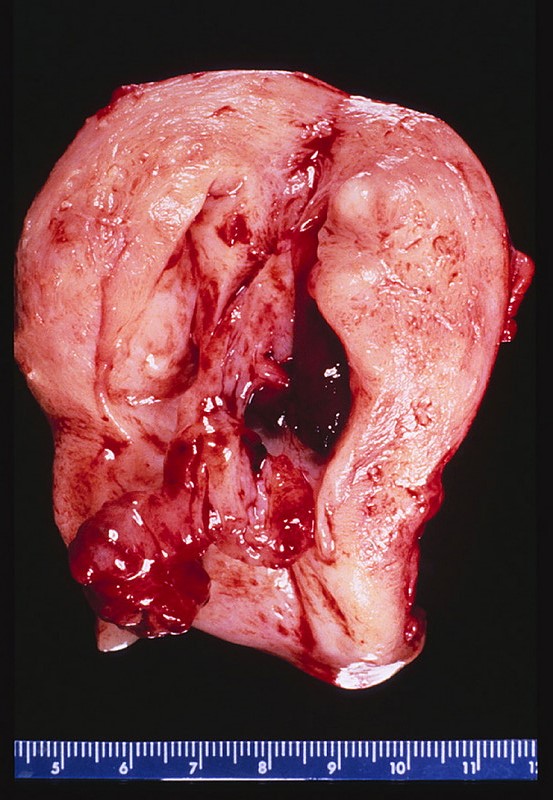
Clinical History: A 58-year-old woman presented to her gynecologist with a two-year history of uterine prolapse and urinary incontinence. A hysterectomy was performed.
(Summary of Gross Findings - click here)
The uterus was slightly enlarged, and contained many gray firm circumscribed nodules 0.5 cm - 2 cm in size. These nodules bulged out of the cut surface. Most of them were located intramurally, but there were some are located in the sub mucosal or the subserosal areas.
|
(Summary of Microscopic Findings - click here)
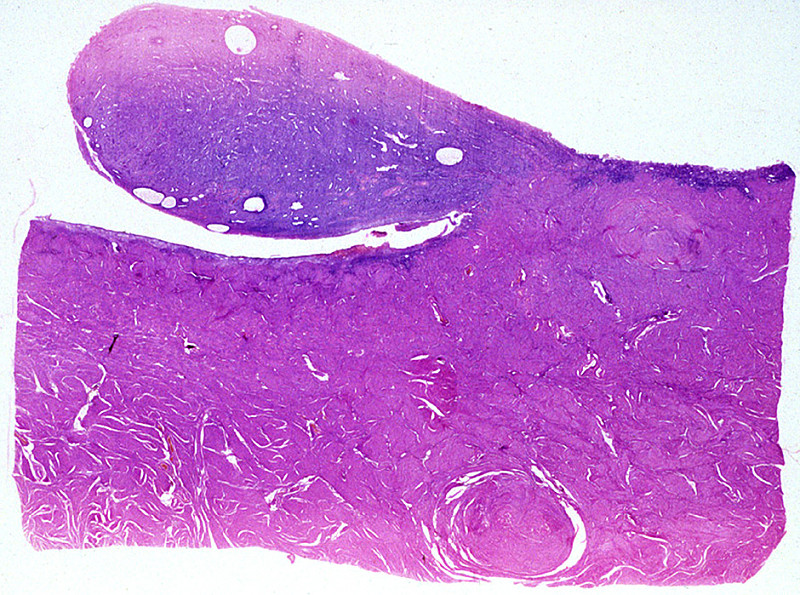
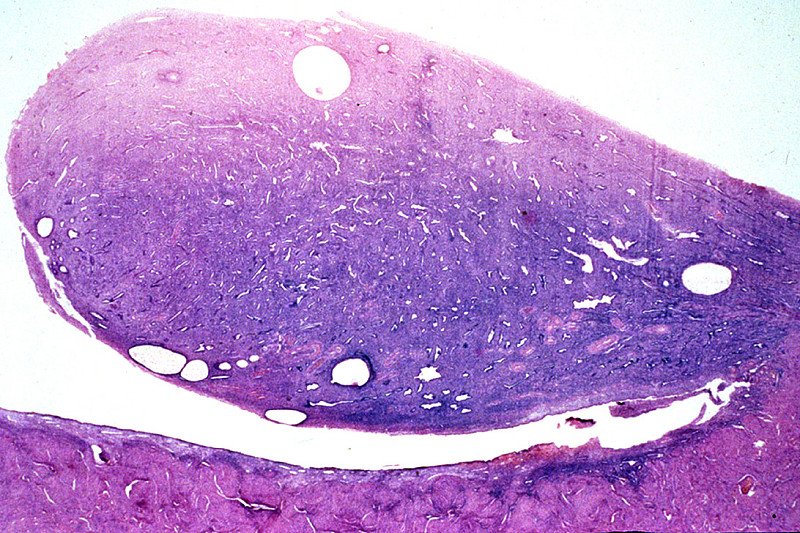
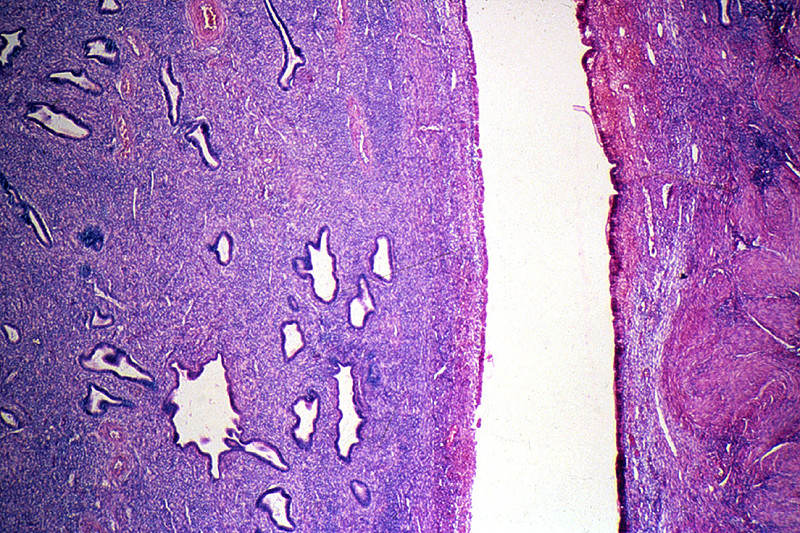
The tumor nodules are composed of interlacing bundles of cells, which have long spindle nuclei and pink fibrillary cytoplasm. These cells resemble the smooth muscle cells of the myometrium. Portions of the tumor tissue have become pink hyalinized masses in which only a few cells are present. These tumor nodules do not have a definite capsule, though their outlines are rather distinct. A small number of vessels are present within the tumor.
|
(Review Normal Histology - click here)
Norm No. 21 Uterus
[ImageScope] [WebScope]
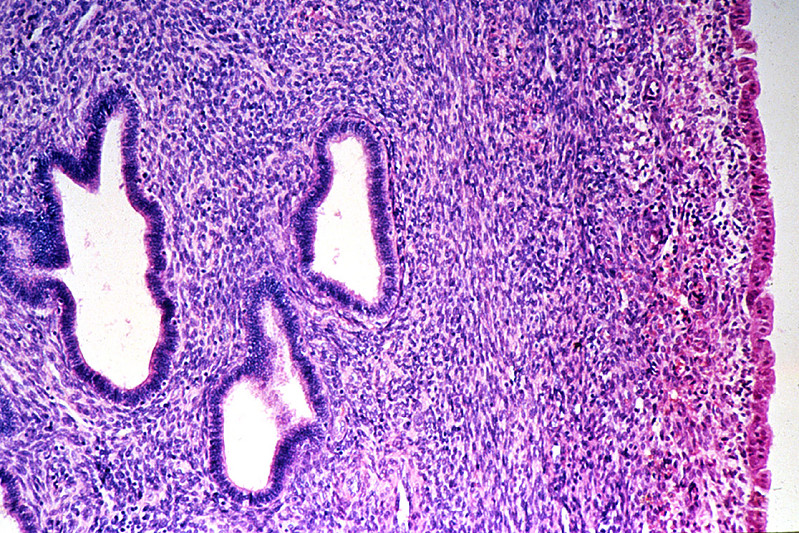
The uterus is a reproductive organ, capable of enormous growth during pregnancy. It is composed of an inner endometrium which supports the placenta during pregnancy. The glandular endometrium undergoes monthly cycles in response to endocrine influence. It undergoes proliferation and then a secretory phase when it is capable of supporting a fertilized ovum. It is subsequently shed during menstruation. The endometrial here is proliferative. If you look carefully you can see mitotic figures in the endometrial glands. Note the regular spacing and orderly array of the endometrial glands. Beneath the endometrium is the myometrium which is composed of smooth muscle cells.
|
220-1. What is the differential diagnosis?
ANSWER
220-2. Which of the following are the proliferating cells in this tumor?
- Endometrial epithelium
- Endometrial stromal cells
- Fibroblasts
- Smooth muscle cells
- Nerves
ANSWER
220-3. Which of the following is the most common presenting sign for this tumor?
- Abdominal mass
- Dyspareunia
- Menorrhagia
- Pelvic pain
- Urinary incontinence
ANSWER
220-4. The presence of which of the following would be most worrisome for malignancy in this tumor?
- Brisk mitotic activity
- Calcification
- Multifocality
- Pedunculation
- Subserosal location
ANSWER
CASE NUMBER 70
[ImageScope] [WebScope]
Clinical history: A 63-year-old woman presented to her physician with a four-week history of intermittent vaginal bleeding. Clinical history revealed that she experienced menopause at age 53 and that five years earlier she received tamoxifen as part of her treatment for breast cancer. A hysterectomy was performed.
Image Gallery:
(Summary of Gross Findings - click here)
The surgical specimen was an enlarged uterus, distorted by multiple firm, grayish-white nodes and nodules (myomata). Within the endometrial cavity was a pedunculated grayish-red mass with smooth surfaces, measuring about 2.5 x 1 cm, lying in the long axis of the uterus.
|
(Summary of Microscopic Findings - click here)
A pedunculated, endometrial polyp arises from the endometrial surface. It is composed of distorted endometrial glands of various sizes, some of which show cystic dilatation. The glands are lined by one or more rows of cells with uniform oval or round nuclei and scanty, eosinophilic cytoplasm. The lumina contain a small amount of mucoid secretions. The surrounding stroma shows slight diffuse, lymphocytic infiltration. The endometrium adjacent to the polyp shows pressure atrophy and focal hemorrhages. Located submucosally and within the myometrium are two small leiomyomas.
|
(Review Normal Histology - click here)
Norm No. 21 Uterus
[ImageScope] [WebScope]
The uterus is a reproductive organ, capable of enormous growth during pregnancy. It is composed of an inner endometrium which supports the placenta during pregnancy. The glandular endometrium undergoes monthly cycles in response to endocrine influence. It undergoes proliferation and then a secretory phase when it is capable of supporting a fertilized ovum. It is subsequently shed during menstruation. The endometrial here is proliferative. If you look carefully you can see mitotic figures in the endometrial glands. Note the regular spacing and orderly array of the endometrial glands. Beneath the endometrium is the myometrium which is composed of smooth muscle cells.
|
70-1. What is the differential diagnosis?
ANSWER
70-2. Which of the following is most strongly associated with development of this lesion?
- History of breast cancer
- Obesity
- P53 mutation
- Tubal ligation
- Smoking
ANSWER
70-3. The presence of which of the following would be most closely associated with malignant progression in this tumor?
- Cellular atypia
- Cystic dilation
- Pedunculation
- Simple hyperplasia
- Surface ulceration
ANSWER
CASE NUMBER 506 -slide courtesy of UMich
[ImageScope] [WebScope]
Clinical History: A 14-year-old girl presented to her pediatrician with a two-month history of right-sided lower abdominal pain. She also noted that she felt “bloated”. A CT scan revealed an 8-cm cystic right adnexal mass and the patient underwent a salpingo-oophorectomy.
Image Gallery:
(Summary of Gross Findings - click here)
The ovary is enlarged and has a heterogeneous appearance with areas of fleshy, white tissue. Focally, there is a cyst. Notably, there is no grumous, sebaceous material present.
|
(Summary of Microscopic Findings - click here)
There are a variety of mature tissues, including choroid plexus (the papillary structures near the center of the tissue), and squamous epithelium (most of the top edge of the tissue). The immature component is seen best in the lower left quadrant of the slide, where there are several highly cellular “blue” areas at low power. At higher power, there are large numbers of primitive small cells with hyperchromatic nuclei, some of which are arranged in rounded “rosettes” around a central lumen-like space These are neuroblasts, and are by far the most common immature component seen in immature teratomas.
|
(Review Normal Histology - click here)
Norm No. 4 Ovary
[ImageScope] [WebScope]
Ovary tissue consists of stoma which is composed of elongated stromal cells. Within the stoma are oocytes in various stages of development. Most of the oocytes have not been stimulated to mature. These resting oocytes have very large nuclei with prominent nucleoli. There are corpora albicantia in a bland stroma. The Corpus Luteum of Pregnancy is composed of granulosa cells with abundant foamy cytoplasm. The granulosa cells are arranged in complex folds.
|
506-1. What is the differential diagnosis?
ANSWER
506-2.Which of the following features distinguishes a mature from an immature teratoma?
- 5-hydroxytryptamine production
- Abundant sebaceous material
- Brisk mitotic activity
- Necrosis
- Presence of embryonal tissue
ANSWER
506-3. Risk of metastasis in immature ovarian tumor is most closely correlated with which of the following?
- Amount of necrosis
- Degree of nuclear pleomorphism
- Number of mitotic figures per ten high-power fields
- Proportion of immature neuroepithelium
- Serum β-HCG levels
ANSWER
CASE NUMBER 123
[ImageScope] [WebScope]
Clinical History: A 25-year-old woman presented to her gynecologist with a three-week history of pelvic pain, fever, and vaginal discharge. On physical examination, she had lower abdominal adnexal tenderness and a painful, swollen left knee. Laboratory studies showed a WBC count of 11,875/mm3 with 68% segmented neutrophils, 8% bands, 18% lymphocytes, and 6% monocytes. She underwent a right salpingo-oophorectomy.
Image Gallery:
(Summary of Gross and Lab Findings - click here)
The uterine tubes were markedly distended and thickened with adhesions between the fimbriated end and the ovaries. On sectioning, pus exuded from the lumen. Cultures grown in chocolate agar and Thayer-Martin agar (TMA contains antibiotics that permit the growth of certain species) yielded colonies. The organisms were small gram negative cocci in pairs.
|
(Summary of Microscopic Findings - click here)
The villi are plump and edematous, with marked dilation and congestion of capillaries. The mucosa is heavily infiltrated by polymorphonuclear leukocytes, which have broken through foci of necrotic mucosa, producing the purulent exudate. Besides this acute phase, there are chronic features evidenced by plasma cell, lymphocytic and macrophage infiltration and fibroblastic proliferation. The muscular layers are edematous and infiltrated by acute and chronic inflammatory cells. This probably represents gonorrheal infection, the mucosa being predominantly involved, in contrast to other pyogenic infections which more frequently involve the outer layers and relatively spare the mucosa.
|
(Review Normal Histology - click here)
Norm No. 20 Uterine (fallopian) tube (aka oviduct)
[ImageScope] [WebScope]
The fallopian tube is lined by ciliated columnar epithelium that aid in transport of the ovum to the uterus. The epithelium is arranged in fronds that project into the lumen. The wall consists of smooth muscle and connective tissue.
|
|
123-1. What is the differential diagnosis?
ANSWER
123-2. Which of the following is the most likely complication of this condition?
- Appendicitis
- Ectopic pregnancy
- Endometriosis
- Polycystic ovarian disease
- Preeclampsia
ANSWER
123-3. Which of the following is the most common etiologic agent in this condition?
- Candida albicans
- Chlamydia trachomatis
- Herpes simplex virus-2
- Mycobacterium tuberculosis
- Neisseria gonorrhea
ANSWER
CASE NUMBER 199
[ImageScope] [WebScope]
Clinical History: A 54-year-old woman presented to her primary care physician with a 9-month history of a breast mass. She stated that she had hoped it would go away and therefore had not sought medical care. Mammography revealed microcalcifications and a needle biopsy was performed. Based on the histologic findings, the patient subsequently underwent a simple mastectomy with sentinel lymph node biopsy.
Image Gallery:
(Summary of Gross Findings - click here)
There is inflammation and dimpling of the areola. The cut surface of the resected breast tissue reveals a 3 x 3 x 2 cm firm mass with stellate borders. The center of the mass is firm, scirrhous and white because of the desmoplasia. There are areas of yellowish necrosis in the portions of neoplasm infiltrating into the surrounding breast. Such tumors appear very firm and non-mobile on physical exam.
|
(Summary of Microscopic Findings - click here)
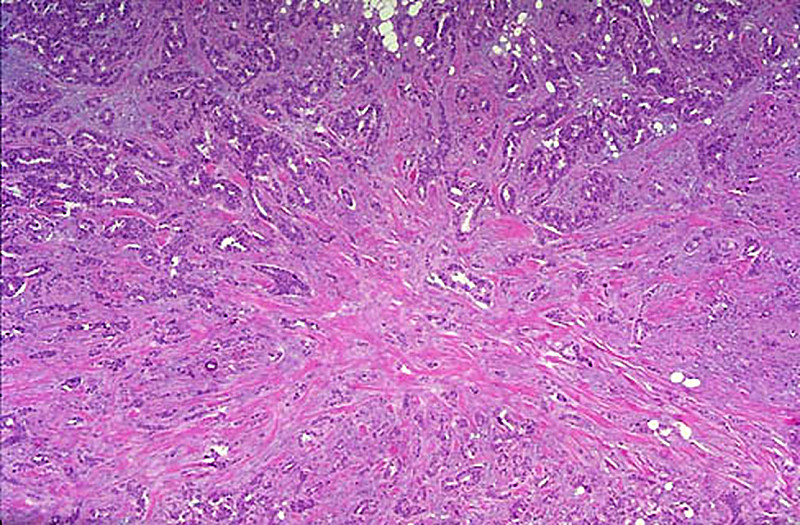
The virtual image was derived from a breast biopsy on another patient and shows both intraductal carcinoma with a comedo pattern of necrosis and invasive infiltrating ductal carcinoma. Ductal carcinomas range from well-differentiated tumors characterized by good duct formation to poorly-differentiated tumors. This one is composed of infiltrating glands and sheets of pleomorphic cells which infiltrate into the adjacent breast tissue. This infiltrating ductal carcinoma of breast at low magnification appears to radiate from a central area of desmoplasia. This collagenous component gives the neoplasm a hard "scirrhous" consistency that is palpable on physical examination or breast self-examination. Such an invasive carcinoma may be fixed to underlying chest wall, making it non-mobile. Also note the nerve which is invaded by tumor. It would also be important for treatment and prognosis to determine if the tumor cells were estrogen and progesterone receptor positive.
|
(Review Normal Histology - click here)
Norm No. 19 Female breast
[ImageScope] [WebScope]
The female breast is a secretory organ that produces milk during lactation. Breast tissue that is not stimulated to lactate consists of resting apocrine cells arranged in nests and small ductules which are lined by cuboidal epithelium. The secretory units are separated from one another by loose connective tissue.
|
199-1. What is the differential diagnosis?
ANSWER
199-2. If the frozen section of the sentinel lymph node is positive for metastatic carcinoma, which of the following should be the next step in the patient’s therapy?
- Bilateral mastectomy and bilateral axillary lymph node dissection
- Complete axillary lymph node dissection and right mastectomy
- Intraoperative radiation of the surgical field
- Right mastectomy alone
- Stop the surgery so the patient can begin neoadjuvant chemotherapy
ANSWER
199-3. Which of the following elements are evaluated in the staging of this tumor?
- Amount of nuclear pleomorphism
- Degree of tubule formation
- Extent of necrosis
- Presence of microcalcifications
- Tumor size
ANSWER
199-4. Five years later, the patient presented with a lytic bone lesion of the right femur. A PET scan shows that the lesion is extremely avid for 18F-fluorodeoxyglucose. A needle biopsy of the patient’s femur lesion showed undifferentiated carcinoma. Which of the following techniques would be the next most logical step to confirm that this is metastatic breast carcinoma?
- DNA microarray analysis
- Flow cytometry
- Fluorescent in situ hybridization
- Immunohistochemistry
- Tissue culture
ANSWER
199-5. Which of the following correlates most strongly with a poor prognosis in invasive breast cancer?
- Dermal lymphatic involvement
- Expression of estrogen and progesterone receptors
- Low tumor stage
- Small tumor size
- Tubular carcinoma histologic type
ANSWER
199-6. In contrast to “luminal A” breast cancer, “luminal B” shows which of the following features?
- Abundant mucinous stroma
- ER positivity
- Her2/neu amplification
- Lower histologic grade
- Lymphoplasmacytic infiltrate
ANSWER
BREAST PATHOLOGY Review Items
Key Vocabulary Terms (click here to search any additional terms on Stedman's Online Medical Dictionary)
LEARNING OBJECTIVES
Absolutely critical information you must know to practice medicine is in bold font.
Important information that will be needed for routine patient care is in regular font.
Information about less common diseases that you may encounter in clinical practice and that will probably appear on examinations is in italics
- Describe the hormonally-induced morphologic changes which occur in the female breast during the following stages:
- neonatal
- pubertal
- menstrual
- gestational
- lactational
- postmenopausal
- Discuss the clinical and pathologic features of the following reactive breast conditions:
- Discuss silicone breast implants, in terms of:
- morphologic changes in adjacent breast
- known epidemiologic relationships with autoimmune disease
- Compare and contrast fibroadenoma and phyllodes tumor in terms of:
- incidence
- clinical presentation
- morphology
- clinical features and prognosis
- Discuss fibrocystic change of the breast in terms of:
- age predilection
- incidence
- etiology
- clinical presentation
- general morphology
- mammographic appearance
- relationship to carcinoma of the breast
- Compare and contrast the clinical and pathologic features of the following morphologic manifestations of fibrocystic change of the breast:
- Compare and contrast the clinical and pathologic features of the following:
- Discuss female mammary carcinoma in terms of:
- genetics
- risk factors
- incidence
- etiology
- pathogenesis
- clinical presentation
- gross morphology
- patterns of spread
- methods of diagnosis
- clinical course
- staging
- prognostic indicators
- treatment options
- survival rates
- Compare and contrast the clinical and pathologic features of the following types of invasive mammary carcinoma:
- Discuss the indications for as well as sensitivity and specificity of the following diagnostic procedures for evaluating breast masses:
- self-examination
- mammography
- fine needle aspiration cytology
- List the most common causes of breast mass in females during the following ages:
- under 35 years of age
- 35-50 years of age
- over 50 years of age
- Compare and contrast the following diseases of the male breast:
FEMALE GENITAL SYSTEM Review Items
Key Vocabulary Terms (click here to search any additional terms on Stedman's Online Medical Dictionary)
LEARNING OBJECTIVES
Absolutely critical information you must know to practice medicine is in bold font.
Important information that will be needed for routine patient care is in regular font.
Information about less common diseases that you may encounter in clinical practice and that will probably appear on examinations is in italics
- Describe the following congenital anomalies and their embryologic bases:
- List the common microorganisms which cause:
- Discuss the clinical and pathologic features of the following vulvar lesions:
- Compare and contrast trichomonal and monilial vaginitis, in terms of:
- predisposing factors
- etiology
- pathogenesis
- symptoms
- methods of detection
- Compare and contrast the clinical and pathologic features of :
- Define discuss general features of extramammary Paget disease, in terms of:
- clinical presentation
- morphology
- associated malignancies
- clinical course
- Discuss vaginal adenosis and vaginal adenocarcinoma, in terms of
- epidemiology
- etiology
- pathogenesis
- morphology
- clinical significance
- Compare and contrast the clinical and pathologic features of cervical lesions:
- Discuss the screening and diagnostic procedures for cervical cancer in terms of methodology, indications, and utilization.
- Discuss cervicovaginal cytology, in terms of:
- technique of obtaining specimen
- utility in diagnosis of inflammatory conditions
- types and significance of abnormalities
- utility in diagnosis of CIN of cervix, carcinoma of cervix and carcinoma of endometrium
- Outline the morphologic effects of oral contraceptive agents (oral contraceptive pills, OCP's) on the endometrium, in relation to mode of action and possible adverse complications.
- Compare and contrast endometriosis and adenomyosis in terms of:
- incidence
- clinical presentation
- pathogenesis
- morphology
- organs involved
- complications
- Discuss the clinical and pathologic features of the following endometrial processes:
- Discuss endometrial carcinoma in terms of:
- incidence
- age distribution
- risk factors
- clinical presentation
- epidemiology
- predisposing factors
- pathogenesis
- morphology including common types
- methods of detection
- grading and staging
- prognosis
- Compare and contrast the clinical and pathologic features of:
- List the conditions which result in non-neoplastic enlargement or cysts of the ovary.
- Discuss polycystic ovarian disease in terms of clinical presentation and morphology.
- Compare and contrast the clinical and pathologic features of ovarian neoplasms:
- surface epithelial tumors
- benign
- borderline
- malignant
- sex cord-stromal tumors
- germ cell tumors
- metastatic malignancy to ovary
- Compare and contrast ovarian vs. placental (gestational) choriocarcinoma, in terms of:
- cell of origin
- pathogenesis
- morphology
- clinical features
- treatment and prognosis
- List the most common primary malignant tumors which metastasize to the ovary.
- List and differentiate among clinical etiologies of:
- pelvic pain in reproductive age group
- vaginal bleeding in reproductive age group
- vaginal bleeding in post-menopausal age group
- vulvar lesions in older women
|