CASE NUMBER 413
[ImageScope] [WebScope]
Clinical History: A 57-year-old man presented to his primary care physician with a 3-month history of back pain and 2-week history of fatigue and weakness. Plain radiograph showed lytic lesions in multiple bones and urinalysis revealed Bence Jones protein. Laboratory analysis showed anemia. A bone marrow biopsy was performed and, based on the diagnosis, chemotherapy and radiation was initiated; however, the patient developed sepsis and died.
Image Gallery:
(Summary of Gross Findings - click here)
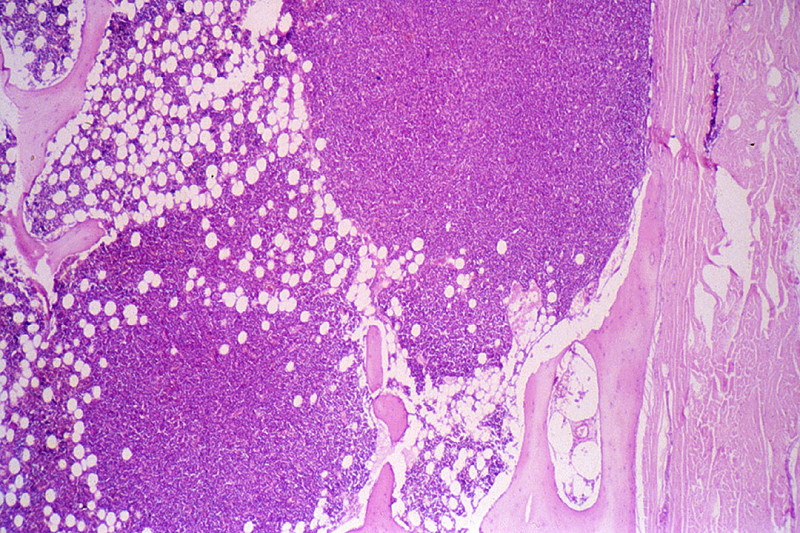
Many of the bones contained poorly delineated, soft gelatinous red tumor masses of various dimensions. Plain film of the skull shows sharply punched out bone lesions.
|
(Summary of Microscopic Findings - click here)
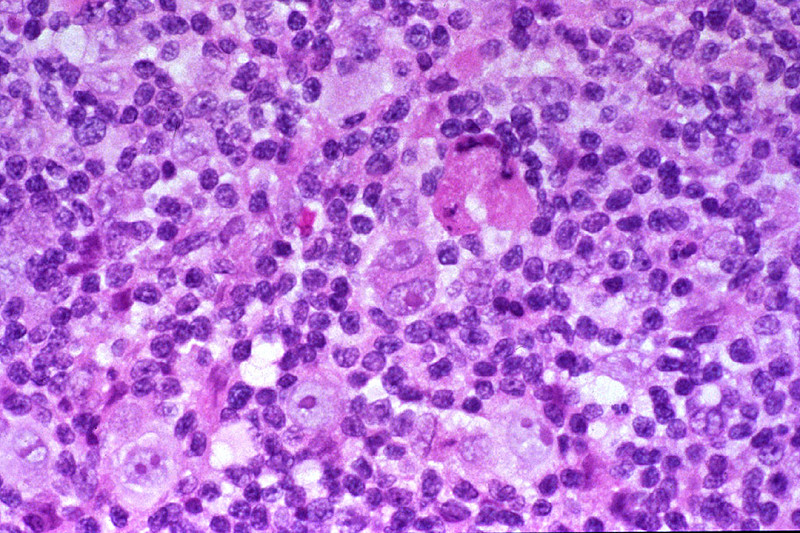
The marrow is heavily infiltrated with plasma cells which vary in degree of maturation. Islets of normoblasts are present, but granulocytes and megakaryocytes are markedly decreased. There is considerable loss of trabecular and cortical bone.
|
(Review Normal Histology - click here)
Specimen No. 67. Bone marrow, human, H&E
[ImageScope] [WebScope]
A thin layer of compact/dense bone borders this section, with internal cancellous/spongy bone. The spaces between bony spicules are filled with hematopoietic cells. Not the large numbers of (round, empty) fat cells present within the marrow space. The fat is lost during processing into paraffin sections. Megakaryocytes can be readily identified, since they are approximately 5-fold larger than most bone marrow cells and contain strongly eosinophilic cytoplasm and multiple nuclei.
(slide and description courtesy of Dr. Laura Hale, Duke PATHOL725 course director)
|
413-1. Which of the following is the most likely diagnosis?
- Diffuse large B-cell lymphoma
- Ewing sarcoma
- Metastatic carcinoma
- Multiple myeloma
- Plasmacytoma
413-2. Which of the following additional findings is most likely in this patient?
- Abundant pulmonary histiocytes
- Amyloidosis
- Multiple cutaneous lesions
- Polycythemia
- Thrombocytosis
413-3. Which of the following is true regarding this disease?
- IgM is the most common serum Ig
- Most patients live >10 years after diagnosis
- Renal insufficiency is rarely the cause of death
- Soft tissue involvement can be seen in advanced disease
- Transformation to diffuse large B cell lymphoma is seen in 25% of patients
413-4. Which of the following chromosomal alterations is associated with this disease?
- ALK rearrangements
- del 13q14.3
- Hyperploidy
- (11; 14) translocation
- (14; 18) translocation
CASE NUMBER 295
[ImageScope] [WebScope]
Clinical History: A 16-year-old boy presented to his pediatrician with a 3 cm mass on right side of his neck. This mass was biopsied. Following diagnosis, a screening CT was performed and revealed a mediastinal mass.
Image Gallery:
(Summary of Gross Findings - click here)
The lymph node was enlarged, and remarkable for fibrous bands separating areas of firm, fleshy material.
|
(Summary of Microscopic Findings - click here)
The normal lymph node architecture is completely destroyed. In its place are thick bands of collagen, separating islands of lymphoid tissue. In some of these nodules, there is a mixed infiltrate consisting of lymphocytes, eosinophils, some neutrophils and plasma cells, and numerous large cells with highly pleomorphic nuclei. Nuclei are frequently multi lobulated but classic binucleate Reed-Stemberg cells are uncommon. Many cells are so-called "lacunar variants", with nuclei which have artefactually shrunken away from their cytoplasmic borders, leaving a clear space than can often easily be appreciated at low power.
|
(Review Normal Histology - click here)
Norm No. 29 Lymph node
[ImageScope] [WebScope]
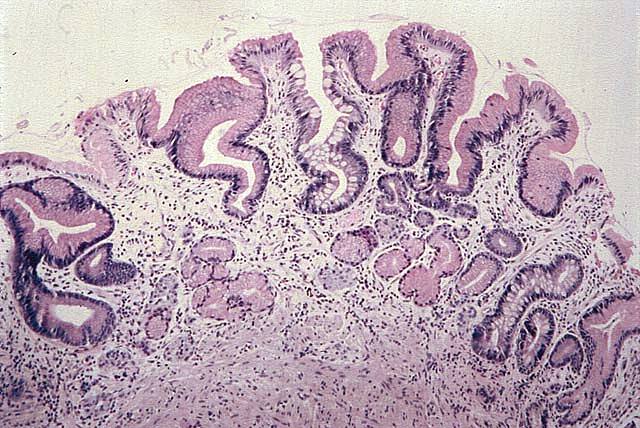
The lymph node contains a cortex which includes the lymphoid follicles and a medulla which is looser tissue containing the lymphatic channels and blood vessels.
|
295-1. Which of the following is the most likely diagnosis?
- Acute myeloid leukemia
- Burkitt lymphoma
- Diffuse large B-cell lymphoma
- Mantle cell lymphoma
- Nodular sclerosis Hodgkin lymphoma
295-2.Which of the following is true regarding this disease?
- Epstein-Barr virus infection is common
- It is the least common subtype in this family of diseases
- Lacunar cells are diagnostic
- Males are more commonly affected than females
- Most patients present with Stage III disease or higher
CASE NUMBER 508
(no virtual slides for this case)
Clinical History: A 65-year-old African-American man presented to his primary care physician with a one-month history of fatigue and weakness and a 10-pound weight loss. Physical exam revealed pale mucous membranes and a reddened, smooth tongue. Laboratory analysis showed an increased MCV and a decreased hematocrit. A bone marrow smear, peripheral blood smear, and a subsequent gastric biopsy are provided for evaluation (NORMAL marrow smears are provided in the first two panels for comparison).
Image Gallery:
508-1. Which of the following is the most likely diagnosis?
- Hereditary spherocytosis
- Iron deficiency anemia
- Malaria
- Megaloblastic anemia
- Sickle cell anemia
508-2. Which of the following is the most appropriate treatment?
- Bone marrow transplant
- High dose vitamin B12
- Iron supplementation
- Monthly blood transfusions
- Splenectomy
508-3. Which of the following is the most common cause of this condition?
- Chronic renal failure
- Infection with parvovirus B19
- Iron deficiency
- Pernicious anemia
- Trauma to red blood cells
508-4. This patient has an increased risk of developing which of the following?
- Aortic aneurysm
- Cirrhosis of the liver
- Diffuse large B-cell lymphoma
- Gastric carcinoma
- Splenic infarction
CASE NUMBER 513
(no virtual slides for this case)
Clinical History: A 29-year-old woman who was diagnosed with celiac disease 6 months earlier presents to her primary care physician with a 3-week history of fatigue and dizziness. She states that she has not followed her doctor’s dietary recommendations. Physical exam was significant for noticeable pallor. Laboratory analysis showed a hemoglobin of 7 gm/dL, serum ferritin of 10 nanograms/mL and an RDW of 20%. A peripheral smear is shown below.
Image Gallery:
513-1. Which of the following is the most likely diagnosis?
- Anemia of chronic disease
- Folate deficiency anemia
- Immunohemolytic anemia
- Iron deficiency anemia
- Vitamin B12 deficiency anemia
513-2. This patient’s decreased iron levels are most likely due to which of the following?
- Decreased hepcidin production
- Decreased transferrin levels
- Dihydrofolate reductase inhibition
- Impaired iron absorption
- Occult bleeding due to peptic ulcer disease
513-3. Which of the following is the most common cause of this type of anemia in the Western world?
- Chloramphenicol treatment
- Chronic blood loss
- Rheumatoid arthritis
- Inherited defects of telomerase
- Vegetarian diet
CASE NUMBER 605
(no virtual slides for this case)
Clinical History: A 45-year old woman presents with marked splenomegaly. Her leukocyte count is increased to 300,000/uL. The differential count reveals the presence of small numbers of myeloblasts and promyelocytes, with a predominance of myelocytes, metamyelocytes, bands, and segemented neutrophils. Basophils are also increased in number, as are platelets. The patient is not anemic. Leukocyte alkaline phosphatase is decreased. The peripheral blood film is shown.
Image Gallery:
605-1. What is the most likely diagnosis?
- Chronic lymphocytic lymphoma
- Multiple myeloma
- Hairy cell leukemia
- Chronic myelogenous leukemia
- Acute myelogenous leukemia
605-2. Which of the following describes a major characteristic of this disorder?
- Chr 9;22 translocation
- Expansion of mature B Lymphocytes within multiple lymph nodes
- Hypogammaglobulinemia
- Neoplastic cells exhibiting hair-like filamentous projections
- Peak incidence at 65 years of age
She undergoes chemotherapy with imatinib mesylate (tyrosine kinase inhibitor), which reduces the spleen size and brings the total leukocyte count within normal range. She remains in remission for 3 years and then begins to experience fatigue and a 10-kg weight loss. Physical examination now shows petechial hemorrhages. CBC shows hemoglobin of 10.5 g/dL, hematocrit 30%, platelet count 60,000 µL, and WBC count 40,000/µL. A peripheral blood smear is shown. Karyotypic analysis shows two Ph1 chromosomes and aneuploidy. Flow cytometric analysis of the peripheral blood shows CD19+, CD10+, sIg-, CD3- cells.
605-3. Which of the following complications of the initial disease did this patient develop following therapy?
- Sézary syndrome
- Myelodysplastic syndrome
- Hairy cell leukemia
- B-lymphoblastic leukemia
- Acute myeloblastic leukemia
CASE NUMBER 606
(no virtual slides for this case)
Clinical History: A 3-year old boy presents with epistaxis and fever. Multiple cutaneous petechiae are evident, and there is generalized enlargement of lymph nodes, as well as palpable splenomegaly. The hemoglobin and platelet count are markedly decreased, and the white blood cell count is elevated to 40,000 cells/uL, with a preponderance of lymphoblasts. The peripheral blood film is shown.
Image Gallery:
606-1. What is the most likely diagnosis?
- Chronic lymphocytic lymphoma
- Acute lymphocytic leukemia
- Hairy cell leukemia
- Chronic myelogenous leukemia
- Acute myelogenous leukemia
606-2. Which of the following statements best characterizes this disorder?
- It is the form of acute leukemia that is most responsive to therapy
- It occurs most often in adults but can occur in children
- Lymphoblastic cells cause damage to normal blood cells, resulting in low cell counts
- The presence of the CD10 marker is indicative of a poorer prognosis
606-3. He receives a course of chemotherapy and achieves a complete remission. Which of the following combinations of phenotypic and karyotypic markers is most likely to be present in this patient?
- Early pre-B (CD19+, CD10+, TdT+); hyperdiploidy
- T cell (CD3+, CD2+, TdT+); normal karyotype
- Pre-B (CD19+, CD10+, TdT+, Cµ+); t(9;22)
- Early pre-B (CD19+, CD10+, TdT+); t(9;22)
- Pre-B (CD19+, CD10+, TdT+, Cµ+); normal karyotypes
HEMATOPATHOLOGY Review Items
Key Vocabulary Terms (click here to search any additional terms on Stedman's Online Medical Dictionary)
LEARNING OBJECTIVES
Absolutely critical information you must know to practice medicine is in bold font.
Important information that will be needed for routine patient care is in regular font.
Information about less common diseases that you may encounter in clinical practice and that will probably appear on examinations is in italics
- Define and state the significance of each of these peripheral blood smear findings:
- Define and state the significance of each of the following cells on a bone marrow smear:
- Explain:
- the concept of reference (normal) range
- the theory of the automated cell counter
- the components of the complete blood count (CBC)
- CBC application in patient evaluation
- Compare and contrast the reporting of leukocyte differential counts as relative percentages vs. absolute numbers, in terms of the advantages and disadvantages of each system.
- Discuss the stages of erythropoiesis in terms of:
- morphology of each stage
- stages in which hemoglobin is produced
- lifespan of reticulocytes and mature red blood cells
- mechanisms of degradation of senescent erythrocytes
- factors (vitamin, minerals and hormones) which influence erythropoiesis
- Discuss the stages of granulopoiesis in terms of:
- morphology of each stage
- time to form and life span of mature granulocytes
- basic functions of the different types of maturing granulocytes
- factors which influence granulopoiesis.
- Discuss the stages of development of lymphocytes, plasma cells, and monocytes, in terms of:
- morphology
- life span of mature forms
- functions of mature forms
- factors which influence production.
- Discuss thrombocytopoiesis in terms of:
- morphology of megakaryocytes
- fate of megakaryocytes
- life span of platelets
- factors which influence thrombocytopoiesis
- abnormal morphologic forms of platelets and megakaryocytes
- Discuss the following classification of anemia in terms of rationale for its use, and specific examples in each category:
- Categorize and discuss laboratory test procedures used in the diagnosis of anemia, outlining the basic workup of a patient who presents with anemia.
- Assess bone marrow function in the diagnosis of the anemic patient, on the basis of:
- reticulocyte count (relative, absolute, and corrected)
- serum bilirubin
- urobilinogen concentration
- Discuss the clinical and pathologic features of the following types of anemia:
- Utilize peripheral blood and bone marrow smears to assess the deviations from normal marrow response which occur in:
- hemolytic anemias
- nuclear maturation defects
- cytoplasmic maturation defects
- hypoproliferative anemias
- Compare and contrast anemia secondary to acute vs. chronic blood loss
- etiology
- pathophysiologic changes
- clinicopathologic diagnosis
- Discuss the clinical and pathologic features of these types of anemia:
- Compare and contrast warm vs. cold antibody immunohemolytic anemias in terms of:
- etiology
- pathogenesis
- associated risks-diseases
- laboratory diagnosis
- clinical features and course
- Compare and contrast intravascular vs. extravascular hemolysis, in terms of:
- etiology
- pathogenesis
- laboratory diagnosis
- clinical findings and course
- Compare and contrast clinical and pathologic features of :
- Describe the WHO classification of acute myeloblastic leukemias in terms of:
- nomenclature
- incidence of each type
- general features of each type
- List the major etiology and pathogenesis of the following:
- Distinguish between leukemia and leukemoid reaction on the basis of:
- etiology
- pathogenesis
- laboratory data
- Morphologically differentiate a blast from a monocyte and lymphocyte.
- Discuss the clinical and pathologic features of these myelodysplastic syndromes:
- Define and classify the myeloproliferative disorders.
- Discuss the clinical and pathologic features of these myeloproliferative disorders:
- Compare and contrast the clinical and pathologic features of:
- Describe the proper mode of submission of a lymph node biopsy to the surgical pathology laboratory for workup of a suspected lymphoproliferative disorder.
- Define, state the significance of, and identify in a microscopic section of a lymph node or extranodal site of involvement each of the following:
- Compare and contrast the clinical and pathologic features of follicular hyperplasia and follicular lymphoma.
- Discuss general features of non-Hodgkin lymphoma in terms of:
- incidence
- immunophenotyping (T vs B cells)
- morphologic patterns (diffuse vs. follicular)
- principles of:
- classification (WHO)
- grading
- staging
- laboratory methods of diagnosis
- clinical features
- prognosis
- extra lymphatic organs involved
- likelihood of a leukemic phase
- Compare and contrast the clinical and pathologic features of :
- Compare and contrast clinical and pathologic features of:
- Discuss Hodgkin lymphoma in terms of:
- Compare and contrast the clinical and pathologic features of :
- Discuss clinical and pathologic features of:
- List benign and malignant etiologies of lymphadenopathy and splenomegaly.
- Categorize and discuss the different types of plasma cell dyscrasias in terms of definitions and clinical presentation.
- Discuss clinical and pathologic features of multiple myeloma.
- Discuss clinical and pathologic features of Waldenström macroglobulinemia.
- Compare and contrast the clinical and pathologic features of:
- Discuss the different laboratory procedures used in the clinicopathologic diagnosis of the different plasma cell dyscrasias.
- List benign and malignant etiologies of monoclonal gammopathies.
- Discuss the clinical and pathologic features of Langerhans cell histiocytosis.
- Classify major causes of changes in size of the spleen, either increasing OR decreasing.
- Discuss Hodgkin lymphoma in terms of:
|
|
|
|
- extramedullary hematopoiesis
|
|
|
|
- List the major complications of splenomegaly.
- Briefly describe the morphologic features and clinical findings in:
- Discuss thrombocytopenia in terms of:
- differential diagnosis
- clinical features
- bone marrow morphology and
- laboratory features
- Discuss thrombocytosis in terms of diagnosis and differential diagnosis.
- Outline the role of platelets in normal hemostasis.
- Outline the process for stepwise evaluation of a patient with suspected platelet disorder.
- Compare and contrast the following disorders of platelets the clinical and pathologic:
- Categorize and discuss acquired disorders of platelet function.
- Compare and contrast clinical and pathologic features of:
- List and discuss the laboratory diagnostic procedures used to approach patients with:
- bleeding disorders
- thrombotic disorders
- Discuss the pathophysiology of disseminated intravascular coagulopathy (DIC).
|