CASE NUMBER 508 - slide courtesy of the University of British Columbia [ImageScope] [WebScope]
Clinical History: A 65-year-old African-American man presented to his primary care physician with a 6-month history of fatigue and weakness and a 2-month history of a burning/tingling sensation in both feet. Physical exam revealed pale mucous membranes and a reddened, smooth tongue. Laboratory analysis showed an increased MCV, a decreased hematocrit and serum antibodies to intrinsic factor. A peripheral smear and a subsequent gastric biopsy are provided for evaluation.
The prominent microscopic finding in this peripheral blood smear is the presence of a neutrophil with a nucleus showing at least seven segments. This is called hypersegmentation. The cytoplasm contains appropriate granules. The red blood cells show mild variation in size (anisocytosis). Some large, oval red blood cells are present, and these oval macrocytes show reduced central pallor. Central pallor is not increased in red cells overall. Platelets appear to have normal morphology.
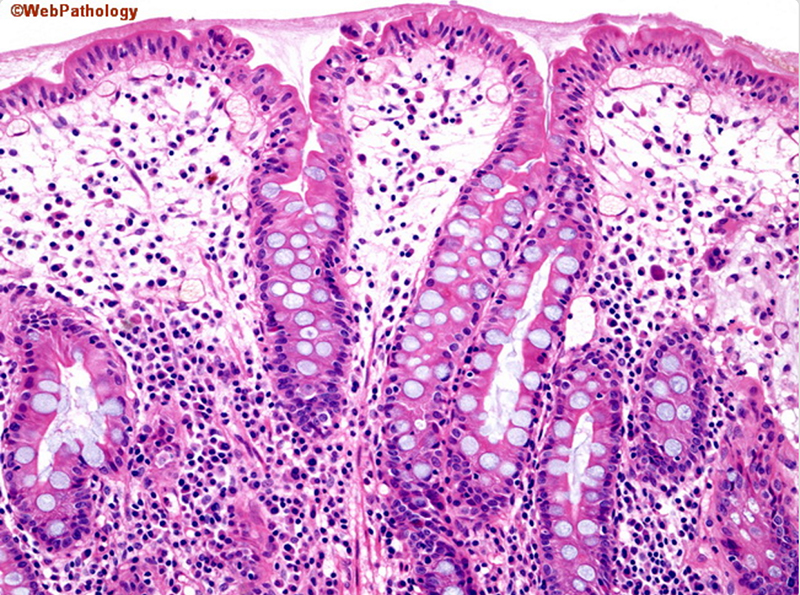
The gastric biopsy shows loss of parietal cells and intestinal metaplasia. There is a deeply seated mixed inflammatory infiltrate consisting of lymphocytes, macrophages and plasma cells.
Scan around the 63x and 86x slides at high magnification to see the various kinds of blood cells that were discussed in the lecture. Most abundant, of course, are the red blood cells (RBCs) or erythrocytes, which are seen in large numbers everywhere you look. In between the RBCs you should look for small, basophilic fragments which are platelets or thrombocytes [example] that are important in blood clotting. As you continue viewing, you will see occasional white blood cells (leukocytes). Some of the white blood cells may defy identification, often because the cells were damaged during slide preparation, so look for characteristic examples, and ignore the equivocal cells. Refer to the images in your texts and from the lecture and try to find an example of each leukocyte type using the 63x and 86x slides (there's less area to cover in these high-mag slides and the cells present are excellent, although the 63x slide does NOT contain any basophils).
The most common white blood cell is the neutrophil, which has a distinct multi-lobed nucleus (often 3-5 lobes). Also frequently seen are lymphocytes, which are small cells (often as small as RBCs) with a dark nucleus and very little cytoplasm. Another cell type is the monocyte, the largest of the blood cells. It has a large, relatively pale nucleus, and rather clear cytoplasm (granules are usually less apparent than those in the illustration in W). You will also see an occasional eosinophil, with prominent reddish granules filling the cytoplasm, and a nucleus with 2 (or sometimes 3) lobes. The exact color of the granules may vary from slide to slide, depending on how well the slide was prepared. In your particular slides they may be anywhere from bright red to dull brown. The remaining cell type you may see on your slides is the basophil, which is hard to find, since it constitutes less than 1% of the leukocytes (the 86x slide actually has THREE excellent examples). The cytoplasm contains large, irregular granules in a "grape-cluster" appearance that usually stain dark blue or almost black. Basophil nuclei may often appear somewhat oval-shaped, so, at first glance, they may be confused with lymphocytes. However, the presence of the large, dark-staining granules should help you distinguish them; also, remember that basophils are rare.
After you've done some looking on your own, here some quick links showing examples of each type of leukocyte (in order of their normal frequency in a blood smear):
Clinical History: A 29-year-old woman who was diagnosed with celiac disease 6 months earlier presents to her primary care physician with a 3-week history of fatigue and dizziness. She states that she has not followed her doctor’s dietary recommendations. Physical exam was significant for noticeable pallor. Laboratory analysis showed a hemoglobin of 7 gm/dL, serum ferritin of 10 nanograms/mL (normal range female 12-150 ng/mL) and an RDW of 20% (normal 11.5-14.5%) . A peripheral smear is shown below.
The red cells show moderate variation in size and shape (aniso-poikilocytosis), including some teardrop cells and oval cells. The central pallor in most red cells is increased (> a third of cell diameter) indicating hypochromia. A lymphocyte is present without significant abnormality. Only four platelets are present in this picture and platelet count may be low, but they show variation in size and the presence of a large platelet indicates active production. (Note: Platelet count is often high in iron deficiency).
Scan around the 63x and 86x slides at high magnification to see the various kinds of blood cells that were discussed in the lecture. Most abundant, of course, are the red blood cells (RBCs) or erythrocytes, which are seen in large numbers everywhere you look. In between the RBCs you should look for small, basophilic fragments which are platelets or thrombocytes [example] that are important in blood clotting. As you continue viewing, you will see occasional white blood cells (leukocytes). Some of the white blood cells may defy identification, often because the cells were damaged during slide preparation, so look for characteristic examples, and ignore the equivocal cells. Refer to the images in your texts and from the lecture and try to find an example of each leukocyte type using the 63x and 86x slides (there's less area to cover in these high-mag slides and the cells present are excellent, although the 63x slide does NOT contain any basophils).
The most common white blood cell is the neutrophil, which has a distinct multi-lobed nucleus (often 3-5 lobes). Also frequently seen are lymphocytes, which are small cells (often as small as RBCs) with a dark nucleus and very little cytoplasm. Another cell type is the monocyte, the largest of the blood cells. It has a large, relatively pale nucleus, and rather clear cytoplasm (granules are usually less apparent than those in the illustration in W). You will also see an occasional eosinophil, with prominent reddish granules filling the cytoplasm, and a nucleus with 2 (or sometimes 3) lobes. The exact color of the granules may vary from slide to slide, depending on how well the slide was prepared. In your particular slides they may be anywhere from bright red to dull brown. The remaining cell type you may see on your slides is the basophil, which is hard to find, since it constitutes less than 1% of the leukocytes (the 86x slide actually has THREE excellent examples). The cytoplasm contains large, irregular granules in a "grape-cluster" appearance that usually stain dark blue or almost black. Basophil nuclei may often appear somewhat oval-shaped, so, at first glance, they may be confused with lymphocytes. However, the presence of the large, dark-staining granules should help you distinguish them; also, remember that basophils are rare.
After you've done some looking on your own, here some quick links showing examples of each type of leukocyte (in order of their normal frequency in a blood smear):
Clinical History: A 57-year-old man presented to his primary care physician with a 3-month history of back pain and 2-week history of fatigue and weakness. Plain radiograph showed lytic lesions in multiple bones and urinalysis revealed Bence Jones protein. Laboratory analysis showed anemia. A bone marrow biopsy was performed and, based on the diagnosis, chemotherapy and radiation were initiated; however, the patient developed sepsis and died. Radiography, gross and microscopic images are provided.
Many of the bones contained poorly delineated, soft gelatinous red tumor masses of various dimensions. Plain film of the skull shows sharply punched out bone lesions.
The marrow is heavily infiltrated with plasma cells which vary in degree of maturation. Islets of normoblasts are present, but granulocytes and megakaryocytes are markedly decreased. There is considerable loss of trabecular and cortical bone.
A thin layer of compact/dense bone borders this section, with internal cancellous/spongy bone. The spaces between bony spicules are filled with hematopoietic cells. Not the large numbers of (round, empty) fat cells present within the marrow space. The fat is lost during processing into paraffin sections. Megakaryocytes can be readily identified, since they are approximately 5-fold larger than most bone marrow cells and contain strongly eosinophilic cytoplasm and multiple nuclei.
(slide and description courtesy of Dr. Laura Hale, Duke PATHOL725 course director)
Clinical History: A 16-year-old boy presented to his pediatrician with a 3 cm mass on right side of his neck. This mass was biopsied. Following diagnosis, a screening CT was performed and revealed a mediastinal mass. Gross and microscopic images of the neck mass biopsy are provided.
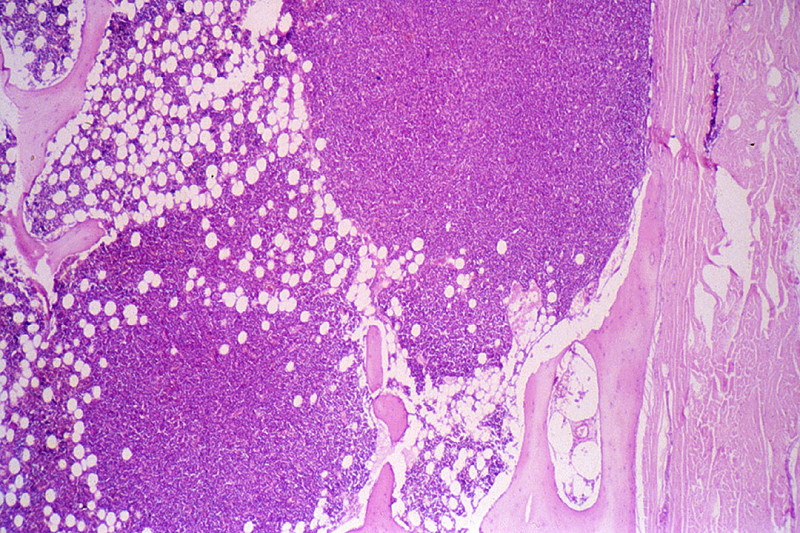
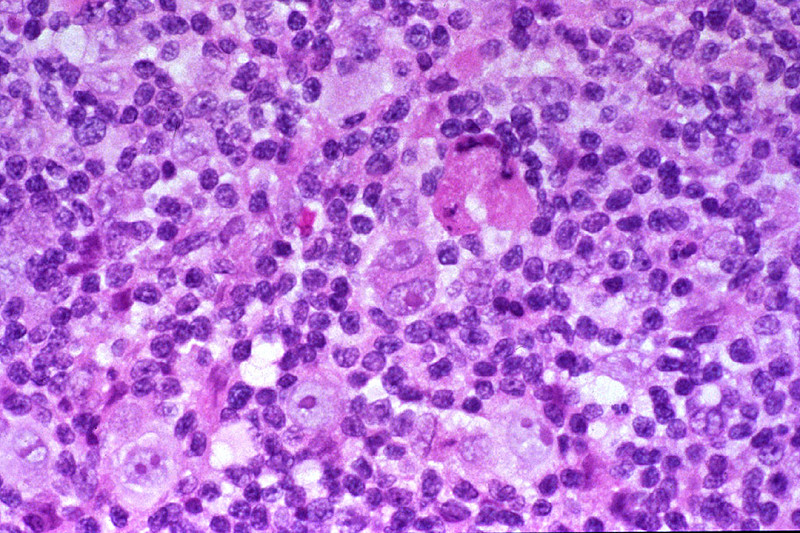
The normal lymph node architecture is completely destroyed. In its place are thick bands of collagen, separating islands of lymphoid tissue. In some of these nodules, there is a mixed infiltrate consisting of lymphocytes, eosinophils, some neutrophils and plasma cells, and numerous large cells with highly pleomorphic nuclei. Nuclei are frequently multi lobulated but classic binucleate Reed-Stemberg cells are uncommon. Many cells are so-called "lacunar variants", with nuclei which have artifactually shrunken away from their cytoplasmic borders, leaving a clear space than can often easily be appreciated at low power.
The lymph node contains a cortex which includes the lymphoid follicles and a medulla which is looser tissue containing the lymphatic channels and blood vessels.
Clinical History: A 3-year old boy presents with epistaxis and fever. Multiple cutaneous petechiae are evident, and there is generalized enlargement of lymph nodes, as well as palpable splenomegaly. The hemoglobin and platelet count are markedly decreased, and the white blood cell count is elevated to 40,000 cells/uL, with a preponderance of lymphoblasts. The peripheral blood film is shown.
Red cells show mild anisocytosis with slight hypochromia. The white cells are all blasts, about 2.5x the diameter of red cells which contain round, oval or slightly indented nuclei containing a fine uniform chromatin and 0-1 small nucleoli. There is a small amount of pale blue, agranular cytoplasm. Platelets are not seen.
Scan around the 63x and 86x slides at high magnification to see the various kinds of blood cells that were discussed in the lecture. Most abundant, of course, are the red blood cells (RBCs) or erythrocytes, which are seen in large numbers everywhere you look. In between the RBCs you should look for small, basophilic fragments which are platelets or thrombocytes [example] that are important in blood clotting. As you continue viewing, you will see occasional white blood cells (leukocytes). Some of the white blood cells may defy identification, often because the cells were damaged during slide preparation, so look for characteristic examples, and ignore the equivocal cells. Refer to the images in your texts and from the lecture and try to find an example of each leukocyte type using the 63x and 86x slides (there's less area to cover in these high-mag slides and the cells present are excellent, although the 63x slide does NOT contain any basophils).
The most common white blood cell is the neutrophil, which has a distinct multi-lobed nucleus (often 3-5 lobes). Also frequently seen are lymphocytes, which are small cells (often as small as RBCs) with a dark nucleus and very little cytoplasm. Another cell type is the monocyte, the largest of the blood cells. It has a large, relatively pale nucleus, and rather clear cytoplasm (granules are usually less apparent than those in the illustration in W). You will also see an occasional eosinophil, with prominent reddish granules filling the cytoplasm, and a nucleus with 2 (or sometimes 3) lobes. The exact color of the granules may vary from slide to slide, depending on how well the slide was prepared. In your particular slides they may be anywhere from bright red to dull brown. The remaining cell type you may see on your slides is the basophil, which is hard to find, since it constitutes less than 1% of the leukocytes (the 86x slide actually has THREE excellent examples). The cytoplasm contains large, irregular granules in a "grape-cluster" appearance that usually stain dark blue or almost black. Basophil nuclei may often appear somewhat oval-shaped, so, at first glance, they may be confused with lymphocytes. However, the presence of the large, dark-staining granules should help you distinguish them; also, remember that basophils are rare.
After you've done some looking on your own, here some quick links showing examples of each type of leukocyte (in order of their normal frequency in a blood smear):
Clinical History: A 45-year old woman presents with marked splenomegaly. Her leukocyte count is increased to 300,000/uL. The differential count reveals the presence of small numbers of myeloblasts and promyelocytes, with a predominance of myelocytes, metamyelocytes, bands, and segemented neutrophils. Basophils are also increased in number, as are platelets. The patient is not anemic. Leukocyte alkaline phosphatase is decreased. The peripheral blood film is shown.
The red cells show two populations some are hypochromic while others are microspherocytic (small and without central pallor). The latter are likely transfused red cells. The white cells are almost all blasts. They vary from 1.5x to 3x the diameter of red cells, have large round to slightly indented nuclei which occupy almost the entire cell (very high nuclear to cytoplasmic ratio). They have fine or reticular nuclear chromatin, 1-3 nucleoli, and a small amount of cytoplasm, which is without granules in most blasts. Platelets are not seen.
Scan around the 63x and 86x slides at high magnification to see the various kinds of blood cells that were discussed in the lecture. Most abundant, of course, are the red blood cells (RBCs) or erythrocytes, which are seen in large numbers everywhere you look. In between the RBCs you should look for small, basophilic fragments which are platelets or thrombocytes [example] that are important in blood clotting. As you continue viewing, you will see occasional white blood cells (leukocytes). Some of the white blood cells may defy identification, often because the cells were damaged during slide preparation, so look for characteristic examples, and ignore the equivocal cells. Refer to the images in your texts and from the lecture and try to find an example of each leukocyte type using the 63x and 86x slides (there's less area to cover in these high-mag slides and the cells present are excellent, although the 63x slide does NOT contain any basophils).
The most common white blood cell is the neutrophil, which has a distinct multi-lobed nucleus (often 3-5 lobes). Also frequently seen are lymphocytes, which are small cells (often as small as RBCs) with a dark nucleus and very little cytoplasm. Another cell type is the monocyte, the largest of the blood cells. It has a large, relatively pale nucleus, and rather clear cytoplasm (granules are usually less apparent than those in the illustration in W). You will also see an occasional eosinophil, with prominent reddish granules filling the cytoplasm, and a nucleus with 2 (or sometimes 3) lobes. The exact color of the granules may vary from slide to slide, depending on how well the slide was prepared. In your particular slides they may be anywhere from bright red to dull brown. The remaining cell type you may see on your slides is the basophil, which is hard to find, since it constitutes less than 1% of the leukocytes (the 86x slide actually has THREE excellent examples). The cytoplasm contains large, irregular granules in a "grape-cluster" appearance that usually stain dark blue or almost black. Basophil nuclei may often appear somewhat oval-shaped, so, at first glance, they may be confused with lymphocytes. However, the presence of the large, dark-staining granules should help you distinguish them; also, remember that basophils are rare.
After you've done some looking on your own, here some quick links showing examples of each type of leukocyte (in order of their normal frequency in a blood smear):
She undergoes therapy with imatinib mesylate (tyrosine kinase inhibitor), which reduces the spleen size and brings the total leukocyte count within normal range. She remains in remission for 3 years and then begins to experience fatigue and a 10-kg weight loss. Physical examination now shows petechial hemorrhages. CBC shows hemoglobin of 10.5 g/dL, hematocrit 30%, platelet count 60,000 µL, and WBC count 40,000/µL. A peripheral blood film is shown in the virtual slide (UMich_55182nl) and illustrated in the image below. Karyotypic analysis shows two Ph chromosomes and aneuploidy. Flow cytometric analysis of the peripheral blood shows CD19+, CD10+, sIg-, CD3- cells.
Image Gallery:
605-3. Which of the following complications of the initial disease did this patient develop following therapy?
Absolutely critical information you must know to practice medicine is in bold font. Important information that will be needed for routine patient care is in regular font. Information about less common diseases that you may encounter in clinical practice and that will probably appear on examinations is in italics
Define and state the significance of each of these peripheral blood smear findings:
Compare and contrast the reporting of leukocyte differential counts as relative percentages vs. absolute numbers, in terms of the advantages and disadvantages of each system.
Describe the proper mode of submission of a lymph node biopsy to the surgical pathology laboratory for workup of a suspected lymphoproliferative disorder.
Define, state the significance of, and identify in a microscopic section of a lymph node or extranodal site of involvement each of the following: