CASE NUMBER 31
[ImageScope] [WebScope]
Clinical History: A 45-year-old man presented to the emergency department with a 2-hour history of chest pain that radiated to both arms and his neck. Physical exam showed diaphoresis and blood pressure of 160/110 mmHg. He was treated with the diuretic furosemide; however, two days after the onset of his chest pain, he experienced a cardiac arrest and died.
Image Gallery:
(Summary of Gross Findings - click here)
The heart was slightly enlarged weighing 460gms. There was severe atherosclerosis of all the major coronary arteries with a recent thrombotic occlusion of the proximal left anterior descending coronary artery. A recent transmural infarct was present in the left ventricle that involved the interventricular septum and the papillary muscle.
|
(Summary of Microscopic Findings - click here)
The slide includes a transmural section of the left ventricle. Nearly the entire section is involved by infarct. However, there is a thin rim (5 to 10 cell layers) of endocardial myocytes which have survived because of diffusion of oxygen and nutrients from the ventricular cavity. Other viable myocytes can be found around larger blood vessels within the section. The intense hypereosinophilia of the necrotic myocytes can best be appreciated by comparing the thin rim of lighter staining subendocardial myocytes with the deeper cells. Note also the karyolysis that is characteristic of coagulation necrosis. In some areas there is little inflammatory response. This observation is explained by microvascular necrosis which does not allow access of circulating leukocytes to these areas. In other areas, especially in the epicardial half of the infarct, there is an intense acute inflammatory response. Many intact neutrophils can be seen. In addition, there are many nuclear fragments from lysed neutrophils. Macrophage activity is not evident. These features of the inflammatory response indicate that the infarct was approximately three to four days old. Note also that the inflammation extends to the epicardial surface and that there are deposits of fibrin on the epicardium. This is called fibrinous pericarditis. The granular grey material seen within some blood vessels is barium sulfate, which was injected to permit post-mortem study of the coronaries by radiography.
|
(Review Normal Histology - click here)
Norm No. 13 Heart
[ImageScope] [WebScope]
Normal heart tissue sections demonstrate no evidence of fibrosis or hemorrhage. Cardiac myocytes have moderately sized centrally located nuclei. Normal myocytes are not brightly eosinphilic. Normally no inflammation is seen. Normal cardiac myocytes do not show hypertrophy.
|
31-1. What is the differential diagnosis?
ANSWER
31-2. Which of the following BEST reflects the order of events which led to neutrophil infiltration of the myocardium?
- Adhesion, margination, migration through tissues, migration across vessel wall, rolling along vessel wall
- Adhesion, margination, rolling along vessel wall, migration through tissues, migration across vessel wall
- Margination, rolling along vessel wall, adhesion, migration across vessel wall, migration through tissues
- Migration across vessel wall, margination, rolling along vessel wall, adhesion, migration through tissues
- Rolling along vessel wall, adhesion, margination, migration through tissues, migration across vessel wall
ANSWER
31-3. Initial rolling interactions are mediated by which of the following?
- Arachidonic acid metabolites
- Cadherins
- Integrins
- Platelet endothelial cell adhesion molecule (PECAM-1)
- Selectins
ANSWER
CASE NUMBER 54
[ImageScope] [WebScope]
Clinical History: An 18-year-old woman presented to the emergency department with a two-day history of nausea, vomiting and periumbilical and lower abdominal pain. Earlier that day, she experienced shaking chills and fever. Physical exam showed local tenderness and rigidity with rebound pain in the lower abdomen. Laboratory tests revealed a white blood cell count of 21,900/ dL. She underwent an exploratory laparotomy.
Image Gallery:
(Summary of Gross Findings - click here)
The appendix was swollen, dark red, hemorrhagic, and covered by gray-yellow exudate. Serial cross-sections revealed a distended lumen containing hemorrhagic material and a fecalith, which apparently obstructed the lumen.
|
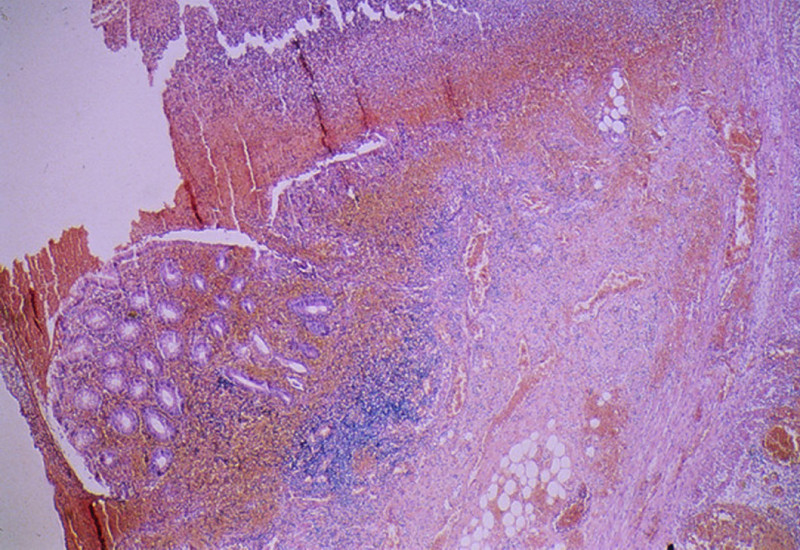
(Summary of Microscopic Findings - click here)
Portions of the mucosa are ulcerated, necrotic and heavily infiltrated with neutrophils. This acute inflammation and necrosis extends throughout the entire thickness of the wall and the serosa. In the lumen of the appendix there is pus and a fecalith.
|
(Review Normal Histology - click here)
Norm No. 8 Appendix
[ImageScope] [WebScope]
The appendix is a tubular organ with a lumen which is lined by mucin secreting columnar epithelium. Although there are generally numerous lymph nodules in the lamina propria and submucosa under normal conditions, there is no evidence of acute inflammation. The submucosa and muscle layers are unremarkable, and there is no inflammation of the serosa.
|
54-1. What is the differential diagnosis?
ANSWER
54-2. The pain experienced by this patient is MOST LIKELY the result of the formation of which of the following two chemical mediators?
- Complement C3b and IgG
- Interleukin-1 and tumor necrosis factor
- Histamine and serotonin
- Prostaglandin and bradykinin
- Leukotriene and HPETE
ANSWER
54-3. One month after the appendectomy, the patient palpates a small nodule beneath the skin at the site of the healed right lower quadrant incision. The nodule is excised, and microscopic examination shows macrophages, collagen, a few small lymphocytes, and multinucleated giant cells. Polarizable, refractile material is seen in the nodule. Which of the following complications of the surgery best accounts for these finding?
- Chronic inflammation
- Abscess formation
- Suture granuloma
- Ulceration
- Edema
ANSWER
CASE NUMBER 51
[ImageScope] [WebScope]
Clinical History: A 45-year-old man was brought by his wife to the emergency room with a one-week history of nausea, vomiting and a high fever. His wife stated that he had been confused since he awakened that morning. Further questioning revealed that he had a history of alcoholism and had been on a drinking spree two weeks earlier. Physical exam revealed dry mucus membranes, an elevated heart rate of 120 bpm, and orthostasis. He was admitted to the hospital for observation and testing, but died suddenly that night.
|
(Review Normal Histology - click here)
Norm No. 24 Lung
[ImageScope] [WebScope]
The primary function of the lung is gas exchange. Therefore, alveoli have thin walls lined by thin flat pneumocytes and endothelial cells. There is no thickening or fibrosis of the interstitium. The bronchioli are lined with basally oriented ciliated columnar epithelium. The bronchi are lined by similar epithelium. There are mucous glands within the submucosa. The bronchial smooth muscle is not hypertrophied. The pulmonary vessels are patent with no evidence of intimal thickening or muscular hyperplasia.
|
|
51-1. What is the differential diagnosis?
ANSWER
51-2. What is the major inflammatory cell type seen in this specimen?
- Macrophages
- Neutrophils
- Mast cells
- Small lymphocytes
- Langhans giant cells
ANSWER
51-3. Which of the following is a feature of chronic inflammation of the lung?
- Edema
- Eosinophilia
- Fibrosis
- Neutrophilic infiltrate
- Vascular congestion and stasis
ANSWER
51-4. The increased vascular permeability demonstrated in this sample is primarily due to the effects of which of the following cell-derived inflammatory mediators?
- Bradykinin
- C3b
- Histamine
- Nitric oxide
- Prostaglandin
ANSWER
CASE NUMBER 123
[ImageScope] [WebScope]
Clinical History: A 25-year-old woman presented to her gynecologist with a three-week history of pelvic pain, fever, and vaginal discharge. On physical examination, she had lower abdominal adnexal tenderness and a painful, swollen left knee. Laboratory studies showed a WBC count of 11,875/mm3 with 68% segmented neutrophils, 8% bands, 18% lymphocytes, and 6% monocytes. She underwent a right salpingo-oophorectomy.
Image Gallery:
(Summary of Gross and Lab Findings - click here)
The uterine tubes were markedly distended and thickened with adhesions between the fimbriated end and the ovaries. On sectioning, pus exuded from the lumen. Cultures grown in chocolate agar and Thayer-Martin agar (TMA contains antibiotics that permit the growth of certain species) yielded colonies. The organisms were small gram negative cocci in pairs.
|
(Summary of Microscopic Findings - click here)
The villi are plump and edematous, with marked dilation and congestion of capillaries. The mucosa is heavily infiltrated by polymorphonuclear leukocytes, which have broken through foci of necrotic mucosa, producing the purulent exudate. Besides this acute phase, there are chronic features evidenced by plasma cell, lymphocytic and macrophage infiltration and fibroblastic proliferation. The muscular layers are edematous and infiltrated by acute and chronic inflammatory cells. This probably represents gonorrheal infection, the mucosa being predominantly involved, in contrast to other pyogenic infections which more frequently involve the outer layers and relatively spare the mucosa.
|
(Review Normal Histology - click here)
Norm No. 20 Uterine (fallopian) tube (aka oviduct)
[ImageScope] [WebScope]
The fallopian tube is lined by ciliated columnar epithelium that aid in transport of the ovum to the uterus. The epithelium is arranged in fronds that project into the lumen. The wall consists of smooth muscle and connective tissue.
|
|
123-1. What is the differential diagnosis?
ANSWER
123-2. Which of the following is a term used to describe the findings in this patient’s WBC?
- Diapedesis
- Eosinophilia
- Leukopenia
- Mastocytosis
- Shift to the left
ANSWER
123-3. Which of the following is the most prominent morphologic pattern of inflammation seen in this case?
- Fibrinous inflammation
- Granulomatous inflammation
- Purulent inflammation
- Serous inflammation
- Ulceration
ANSWER
123-4. Response to this injury will require angiogenesis. Which of the following is the most important factor in this process?
- Elastase
- Interferon gamma
- Matrix metalloproteinase
- TGF-beta
- VEGF
ANSWER
CASE NUMBER 240
[ImageScope] [WebScope]
Clinical History: A 54-year-old man presented to his primary care physician with a one-year history of intermittent upper abdominal pain. Laboratory tests showed mild iron deficiency anemia. Upper endoscopy revealed a solitary ulcerated lesion. Although most cases of this disease are typically treated medically, this patient underwent a partial gastrectomy.
Image Gallery:
(Summary of Gross Findings - click here)
An endoscopic view shows that the gastric mucosa is somewhat flattened but demonstrates a focal ulcer with smooth edges.
|
(Summary of Microscopic Findings - click here)
Microscopic sections show a portion of antral/pyloric stomach. A large ulcer and the accompanying response have replaced all layers of the stomach mucosa and wall. Three layers may be distinguished in the bed of the ulcer. The innermost one is composed of necrotic debris and fibrino-purulent exudate in which bacteria and yeast are present. The middle layer is a zone of granulation tissue made up of small vessels and acute and chronic inflammation. The deepest portion of the ulcer is made up of fibrous scar. Some of the arteries in the scar tissue may show sclerosis. The mucosa adjacent to the ulcer shows acute and chronic gastritis.
|
(Review Normal Histology - click here)
Norm No. 16 Stomach, fundus
[ImageScope] [WebScope]
The normal gastric mucosa of the fundus contains superficial fovea arranged in leaf like fronds and deeper gastric glands. The foveolar cells secrete mucin. The gastric glands include mucous cells, parietal cells, chief cells and enteroendocrine cells.
|
240-1. What is the differential diagnosis?
ANSWER
240-2. In patients with this condition, plain radiographic evidence of free air under the diaphragm in the upright position is most suggestive of which of the following?
- Chronic gastritis
- Frank hemorrhage
- Malignant transformation
- Perforation
- Reactive gastropathy
ANSWER
240-3. The base of this lesion shows dense fibrosis and scarring. Which of the following is the most important factor in the development of these findings?
- Elastase
- Interferon gamma
- Matrix metalloproteinase
- TGF-beta
- VEGF
ANSWER
INFLAMMATION Review Items
Key Vocabulary Terms (click here to search any additional terms on Stedman's Online Medical Dictionary)
LEARNING OBJECTIVES
Absolutely critical information you must know to practice medicine is in bold font.
Important information that will be needed for routine patient care is in regular font.
Information about less common diseases that you may encounter in clinical practice and that will probably appear on examinations is in italics
- Describe vascular changes and cellular events of the inflammatory reaction.
- Discuss the five cardinal signs of inflammation in terms of pathogenesis and underlying morphologic changes.
- Discuss chemical mediators of inflammation, in terms of origin and in vivo function:
- Discuss each of the following in terms of the associated type of inflammation (acute, chronic, or granulomatous) and their role in the inflammatory response:
- Describe the steps involved in the isolation and destruction of an infectious agent by polymorphonuclear leukocytes (neutrophils). Describe important related extracellular and intracellular factors.
- Compare and contrast acute, chronic, and granulomatous inflammation in terms of:
- etiology
- pathogenesis
- histologic appearance
- laboratory findings
- characteristic cells involved
- outcome
- systemic effects
- Compare and contrast resolution, organization and termination of an inflammatory response.
Click here to submit questions or comments about this site.
Duke University | Duke Medicine | School of Medicine | School of Nursing | Doctor of Physical Therapy
Copyright © 2004-2015 Duke University School of Medicine
Updated 2/18/16 - Lippard |