CASE NUMBER 31
[ImageScope] [WebScope]
Clinical History: A 45-year-old man presented to the emergency department with a 2-hour history of chest pain that radiated to both arms and his neck. Physical exam showed diaphoresis and blood pressure of 160/110 mmHg. He was treated with the diuretic furosemide; however, two days after the onset of his chest pain, he experienced a cardiac arrest and died.
Image Gallery:
(Summary of Gross Findings - click here)
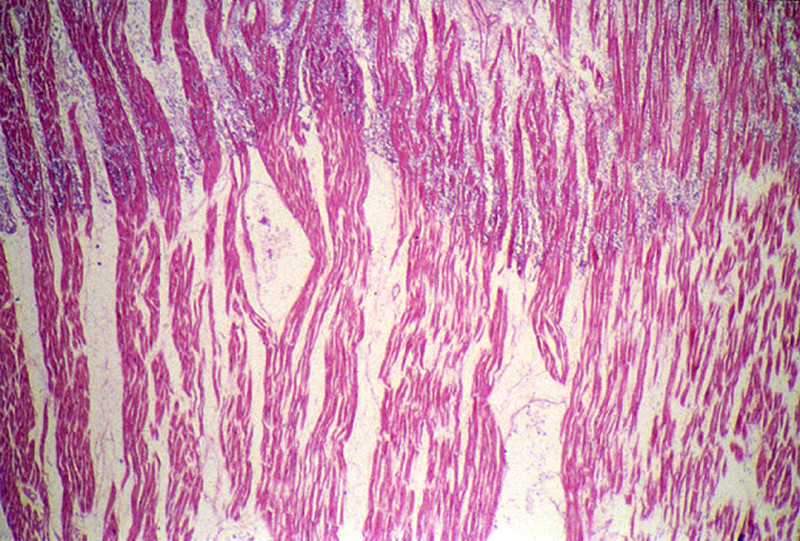
The heart was slightly enlarged weighing 460gms. There was severe atherosclerosis of all the major coronary arteries with a recent thrombotic occlusion of the proximal left anterior descending coronary artery. A recent transmural infarct was present in the left ventricle that involved the interventricular septum and the papillary muscle.
|
(Summary of Microscopic Findings - click here)
The slide includes a transmural section of the left ventricle. Nearly the entire section is involved by infarct. However, there is a thin rim (5 to 10 cell layers) of endocardial myocytes which have survived because of diffusion of oxygen and nutrients from the ventricular cavity. Other viable myocytes can be found around larger blood vessels within the section. The intense hypereosinophilia of the necrotic myocytes can best be appreciated by comparing the thin rim of lighter staining subendocardial myocytes with the deeper cells. Note also the karyolysis that is characteristic of coagulation necrosis. In some areas there is little inflammatory response. This observation is explained by microvascular necrosis which does not allow access of circulating leukocytes to these areas. In other areas, especially in the epicardial half of the infarct, there is an intense acute inflammatory response. Many intact neutrophils can be seen. In addition, there are many nuclear fragments from lysed neutrophils. Macrophage activity is not evident. These features of the inflammatory response indicate that the infarct was approximately three to four days old. Note also that the inflammation extends to the epicardial surface and that there are deposits of fibrin on the epicardium. This is called fibrinous pericarditis. The granular grey material seen within some blood vessels is barium sulfate, which was injected to permit post-mortem study of the coronaries by radiography.
|
(Review Normal Histology - click here)
Norm No. 13 Heart
[ImageScope] [WebScope]
Normal heart tissue sections demonstrate no evidence of fibrosis or hemorrhage. Cardiac myocytes have moderately sized centrally located nuclei. Normal myocytes are not brightly eosinphilic. Normally no inflammation is seen. Normal cardiac myocytes do not show hypertrophy.
|
31-1. Which of the following is the most likely diagnosis?
- Acute myocardial infarct
- Amyloidosis
- Bacterial myocarditis
- Dilated cardiomyopathy
- Hemorrhagic pericarditis
31-2. Which of the following best describes the pathologic findings?
- Caseous necrosis
- Coagulative necrosis
- Fat necrosis
- Fibrinoid necrosis
- Gangrenous necrosis
31-3. Which of the following best describes the nuclear changes seen here?
- Chromatin condensation
- DNA cleavage into nucleosomal subunits
- Karyorrhexis
- Karyolysis
- Pyknosis
31-4. Increased eosinophilia of the dead myocytes is most directly linked to which of the following molecular events?
- Cytoplasmic blebbling
- Denaturation of cytoplasmic proteins
- Increased cytoplasmic RNA
- Generation of myelin figures
- Loss of glycogen particles
31-5. Which of the following are features of necrosis?
- Caspase activation
- Chromatin condensation
- Cytoplasmic blebbing
- DNA cleavage into nucleosomal subunits
- Karyorrhexis
CASE NUMBER 14
[ImageScope] [WebScope]
Clinical History: A 19-year-old female was brought to the emergency department when she was discovered unconscious after she attempted suicide by ingesting about a dozen tablets of mercury bichloride (HgCl2). A small amount of urine obtained in the hospital later that day was positive for occult blood. Although she vomited and was treated aggressively with chelating agents, fluids and colonic irrigation, she became anuric and died 10 days later.
Image Gallery:
(Summary of Gross Findings - click here)
The kidneys were both slightly enlarged but grossly normal.
|
(Summary of Microscopic Findings - click here)
The tubular damage here is so severe that it is hard to identify the segment involved. However, it may be noted that most of the necrosis is in the cortex, whereas the collecting tubules in the medulla, although their lumina contain many casts, are lined by relatively intact cells. HgCl2 presumably damages mainly proximal convoluted tubules because it is concentrated in this segment. Many involved tubules show marked coagulative necrosis, with sloughing of cells into the lumen. Some tubules that look more nearly normal actually have already have undergone marked necrosis and all that is left is a layer of flattened basilar cells which serve to regenerate the tubule. Regenerative changes can be recognized, including occasional mitoses in epithelial cells. The basement membrane around a few necrotic tubules is broken, and the interstitial tissue contains collections of inflammatory cells and edema fluid.
|
(Review Normal Histology - click here)
Norm No. 2 Kidney
[ImageScope] [WebScope]
The kidney excretes soluble waste from the body and controls electrolyte balance. It consists of the cortex and the medulla. Within the outer cortex, glomeruli with delicate capillary loops are seen. The basement membrane is thin and without inflammation or thickening. Bowman’s capsule that surrounds the glomerulus is thin. The interstitium demonstrates no evidence of inflammation or fibrosis. In the areas between the glomeruli, tubules and arterioles are seen. The tubules are intact. The vessels exhibit no narrowing or wall thickening. The inner medulla of the kidney contains only tubules and blood vessels. Larger arteries and veins are located at the interface between cortex and medulla.
|
14-1. Which of the following is the most likely diagnosis?
- Acute tubular necrosis
- Caseous necrosis
- Fibrinoid necrosis
- Gangrenous necrosis
- Liquefactive necrosis
14-2. Since cell injury is typically most prominent where toxin concentrations are highest, which area of the nephron should show the most damage in this patient?
- Distal tubule
- Glomerulus
- Loop of Henle
- Proximal tubule
14-3. Which of the following morphologic changes most likely suggests a diagnosis of acute tubular necrosis?
- Mitochondrial swelling
- Plasma membrane blebs
- Chromatin clumping
- Nuclear fragmentation
- Ribosomal disaggregation
14-4. The case presented here represents irreversible injury (cell death). Which of the following cytologic features is associated with reversible cell injury?
- Liquefactive necrosis
- Nuclear pyknosis
- Swelling of the mitochondria
- Apoptosis
- Lysosome rupture
CASE NUMBER 93
[ImageScope] [WebScope]
Clinical History: A 50-year-old alcoholic man presented to the emergency department with severe epigastric pain that radiated to his back. He stated that he had had multiple similar episodes over the previous five years and had been hospitalized several times for pain management. At this admission, laboratory analysis showed elevated levels of serum amylase and lipase. The patient developed refractory shock, peritonitis and died.
Image Gallery:
(Summary of Gross Findings - click here)
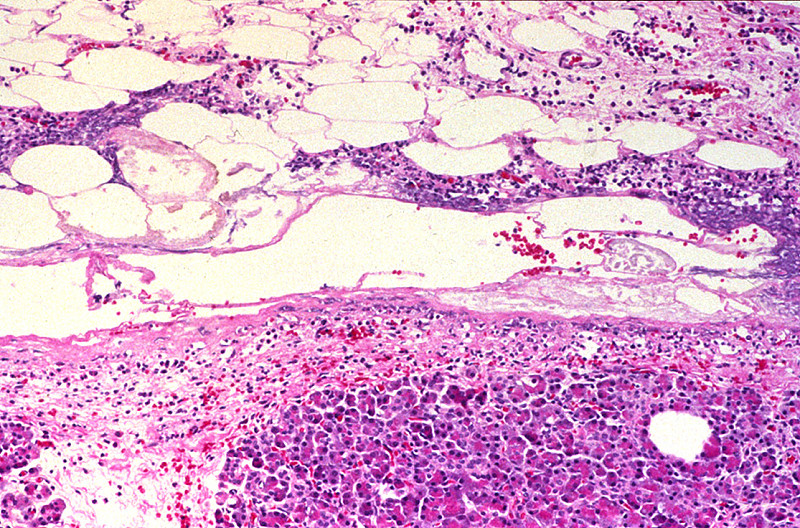
Fibrosis obscured some areas of pancreas architecture. Saponification of peripancreatic fat was seen in small foci.
|
(Summary of Microscopic Findings - click here)
Several areas of fat necrosis with adjacent neutrophil infiltrate are seen, evidence of acute pancreatitis. In addition, some lobules of the pancreas show fibrosis and loss acini, evidence of chronic pancreatitis. In these areas, islets of Langerhans appear larger and more abundant. This is partly because they are resistant to injury and persist when acini are destroyed and partly because they undergo reactive hyperplasia.
|
(Review Normal Histology - click here)
Norm No. 7 Pancreas
[ImageScope] [WebScope]
The pancreas is comprised of glandular tissue with endocrine and exocrine function. The exocrine pancreas contains lobular arrays of acini. The acinar secretions of the exocrine pancreas are collected by the pancreatic ducts. The ducts are surrounded by a small amount of connective tissue without inflammation or fibrosis (scarring).The endocrine pancreas resides in the islets which are regularly arranged and present within the pancreatic lobules.
|
93-1. Which of the following is the most likely diagnosis?
- Acute and chronic pancreatitis
- Lymphoplasmacytic sclerosing pancreatitis
- Pancreatic adenocarcinoma
- Pancreatoblastoma
- Waterhouse-Friderichsen syndrome
93-2. Which of the following pathologic processes is depicted microscopically?
- Cholesterolosis
- Fat necrosis
- Glycogenosis
- Metastatic calcification
- Steatosis
93-3. Which of the following statements is true regarding this disease?
- Cystic fibrosis is the most common cause
- Diabetes mellitus is an early manifestation of this disease
- Disseminated intravascular coagulation is a potential
complication
- Pancreatic adenocarcinoma arises in approximately 25% of patients within 5 years of diagnosis
- There are increased numbers of IgG4-producing plasma cells
CASE NUMBER 95
[ImageScope] [WebScope]
Clinical History: A 60-year-old man presented to the emergency department with severe abdominal pain seven days after a partial colon resection for adenocarcinoma of the colon. A CT scan showed dilated loops of bowel and the patient was taken to surgery for exploratory laparotomy. The patient died while still in surgery.
Image Gallery:
(Summary of Gross Findings - click here)
The jejunum and ileum were dark red, thickened and indurated. The mucosal surface was covered by bloody mucus. The cut surface revealed hemorrhages throughout all layers of the intestinal wall. The superior mesenteric vein and its tributaries were obstructed by dark red thrombi which were attached to the vascular wall.
|
(Summary of Microscopic Findings - click here)
The villi are swollen. The superficial layer of the mucosa is necrotic and contains clumps of bacteria. The deeper layer of the mucosa is hemorrhagic but epithelial cells are relatively well preserved. A severe degree of edema, congestion and hemorrhage is seen throughout the submucosa and muscularis layers. The muscle cells are not yet necrotic.
|
(Review Normal Histology - click here)
Norm No. 17 Jejunum
[ImageScope] [WebScope]
This cross section of the jejunum illustrates the complex mucosal villi and crypts that greatly increase the absorptive surface area.
|
95-1. Which of the following is the most likely diagnosis?
- Campylobacter enterocolitis
- Celiac disease
- Crohn disease
- Hemorrhagic infarct
- Infectious enterocolitis
95-2. A blood sample taken at the time the patient was admitted to the emergency department was submitted for blood culture and grew out a Gram-negative organism. Which of the following is the most likely explanation for this finding?
- Gut bacteria translocated across the intestinal wall
- Infarction of the gut was due to sepsis
- The patient had undiagnosed pneumonia
- The patient is immunosuppressed
- The specimen was contaminated in the emergency department
CASE NUMBER 40
[ImageScope] [WebScope]
Clinical History: A 65-year old man presented to the emergency department with a history of inceasing dyspnea. Physical exam revealed decreased breath sounds, most notably in the lung bases. While under observation, the patient developed severe chest pain and heart palpitations and collapsed in the emergency department. Resuscitation efforts were unsuccessful. Autopsy was requested by the patients wife.
Image Gallery:
(Summary of Gross Findings - click here)
Both lungs were heavy, wet, slightly firm, and dark-red. Frothy clear fluid may be seen on the cut surface.
|
(Summary of Microscopic Findings - click here)
The alveoli are filled with a homogeneous pink material. The septal capillaries are engorged with blood. An incidental finding consists of anthracotic pigment near the pleural space.
|
(Review Normal Histology - click here)
Norm No. 24 Lung
[ImageScope] [WebScope]
The primary function of the lung is gas exchange. Therefore, alveoli have thin walls lined by thin flat pneumocytes and endothelial cells. There is no thickening or fibrosis of the interstitium. The bronchioli are lined with basally oriented ciliated columnar epithelium. The bronchi are lined by similar epithelium. There are mucous glands within the submucosa. The bronchial smooth muscle is not hypertrophied. The pulmonary vessels are patent with no evidence of intimal thickening or muscular hyperplasia.
|
40-1. Which of the following is the most likely diagnosis?
- Atypical pneumonia
- Diffuse alveolar damage
- Interstitial pulmonary fibrosis
- Pulmonary alveolar proteinosis
- Pulmonary edema
40-2. Which of the following is the most common etiology of this condition?
- Cigarette smoking
- Immunosuppression
- Left heart failure
- Microvascular injury
- Right heart failure
40-3. Which of the following is the cause of pulmonary edema in the setting of left-sided heart failure?
- Decreased oncotic pressure
- Impaired surfactant clearance
- Increased hydrostatic pressure
- Injury to the capillaries of the alveolar septa
- Protease release by neutrophils
CASE NUMBER 85: Fatty liver
[ImageScope] [WebScope]
Clinical History: A 64-year-old morbidly obese white woman was admitted to the emergency department with a 6-hour history of nausea, vomiting and jaw pain. While she was in the emergency department she collapsed and died. Autopsy revealed a massive heart attack as well as significant liver pathology.
Image Gallery:
(Summary of Gross Findings - click here)
The liver weighed 1980 grams. It had a pale, greasy appearance.
|
(Summary of Microscopic Findings - click here)
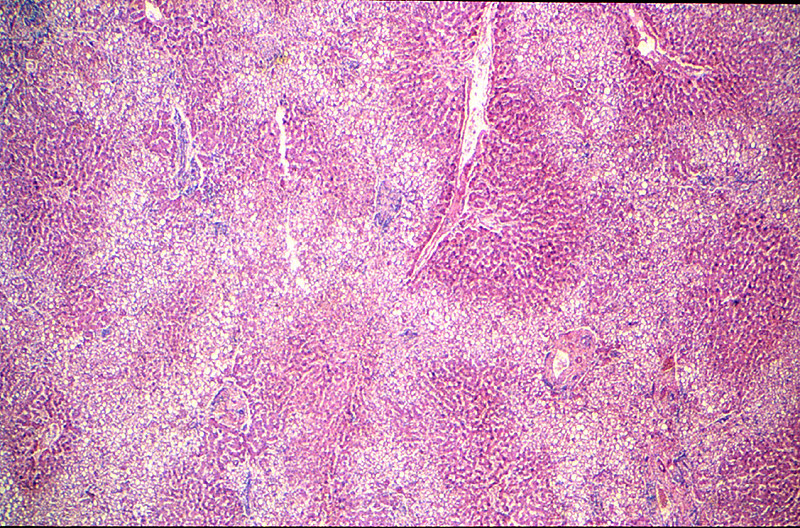
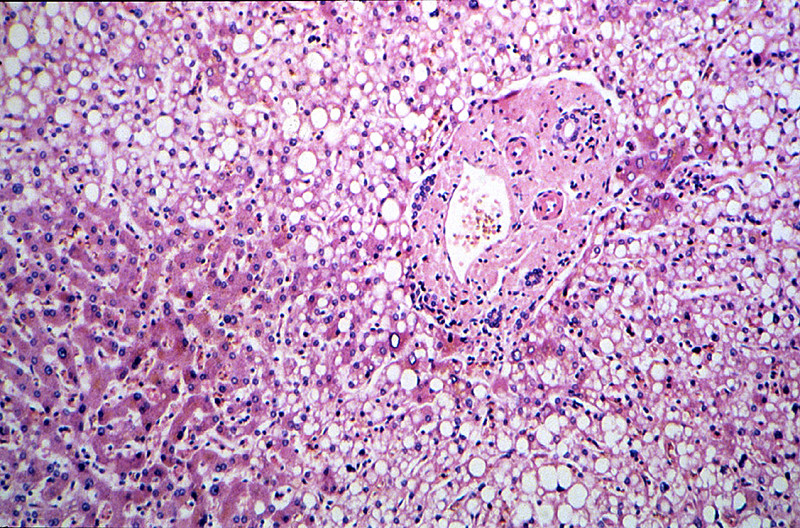
The areas of fatty change are readily visible with use of scanning power. They are zonal. Note the peri-portal areas are severely involved and the areas of fatty change extend from one portal area to another. The more severely involved cells have eccentric nuclei and the entire cytoplasm is replaced by a fat globule.
|
(Review Normal Histology - click here)
Norm No. 3 Liver
[ImageScope] [WebScope]
The liver is the organ that metabolizes nutrients received from the digestive tract. These nutrients and processed by tissue hepatocytes which are large polygonal cells. The hepatocyes are separated by portal triads. The triads consist of an artery, a vein and a bile duct. The bile duct is lined by cuboidal epithelium. The artery has a muscular wall and a flat endothelial lining. The sinuses are well defined and contain a small amount of blood.
|
85-1. Which of the following is the most likely diagnosis?
- Cholesterolosis
- Dystrophic calcification
- Glycogenosis
- Hemochromatosis
- Steatosis
85-2. Which of the following is a common cause of hepatic steatosis in developed nations?
- Alcohol abuse
- Cigarette smoking
- Excess red meat in the diet
- Glucose-6-phosphatase deficiency
- Hepatitis B
85-3. Which of the following is the mechanism by which steatosis is thought to occur?
- Decreased a-glycerophosphate activity
- Impaired fatty acid oxidation
- Increased apoprotein synthesis
- Peripheral sequestration of fatty acids
- Reduced acetate concentration
Review Items
CELL INJURY
Key Vocabulary Terms (click here to search any additional terms on Stedman's Online Medical Dictionary)
| anthracosis |
hemosiderosis |
ischemia |
| aplasia |
heterophagy |
karyolysis |
| apoptosis |
homeostasis |
karyorrhexis |
| atrophy |
hyaline |
lipofuscin |
| autolysis |
hydropic change |
melanin |
| autophagy |
hyperplasia |
metaplasia |
| bilirubin |
hypertrophy |
necrosis |
| dysplasia |
hypoplasia |
neoplasia |
| gangrene |
hypoxia |
pyknosis |
| heat-shock protein |
infarct |
steatosis |
| hemosiderin |
|
|
CELL INJURY LEARNING OBJECTIVES
Absolutely critical information you must know to practice medicine is in bold font.
Important information that will be needed for routine patient care is in regular font.
Information about less common diseases that you may encounter in clinical practice and that will probably appear on examinations is in italics.
- Compare cell and tissue adaptation, reversible cell injury, and irreversible cell injury (cell death) on the basis of:
- etiology
- pathogenesis
- ultrastructural and histologic appearance
- Compare and contrast cell death and somatic death, on the basis of:
- causes
- pathogenesis
- histologic appearance
- Outline the relationships between the following features in terms of changes in the processes of cell injury and death:
- biochemical
- light microscopic
- ultrastructural
- Contrast and compare the clinical and pathologic features of:
- Coagulative necrosis
- liquefactive necrosis
- gangrenous necrosis
- caseous necrosis
- fat necrosis
- fibrinoid necrosis
- apoptosis
- Compare and contrast the following types of cell injury:
- reperfusion
- free radical-induced
- chemical
- understand biochemical and molecular mechanisms
- List the alterations that occur in these subcellular organelles as a consequence of cell injury:
- lysosomes
- endoplasmic reticulum
- mitochondria
- cytoskeleton
- Discuss the significance of intracellular accumulations of:
- lipids
- proteins
- glycogen
- exogenous and endogenous pigments
- Compare fatty change (steatosis) and fatty infiltration on the basis of:
- causes
- pathogenesis
- organs commonly involved
- histologic appearances
- Compare dystrophic and metastatic calcification in terms of:
- definition
- etiology and pathogenesis
- morphologic appearance
- sites and associated diseases
- clinical significance
|