CASE NUMBER 155
[ImageScope] [WebScope] [DigitalScope]
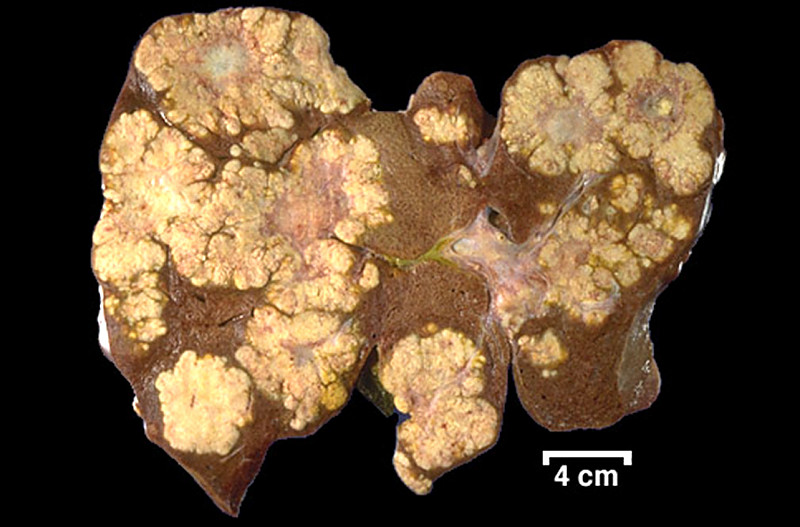
Clinical History: A 72-year-old man with a 5-year history of dementia was admitted to the hospital from a nursing home with fever, mental status changes and productive cough. He was diagnosed with bronchopneumonia and treated with antibiotics, but died in the hospital. An autopsy was performed and the pathologist noted an incidental finding in the liver.
Image Gallery:
(Summary of Gross Findings - click here)
In the right lobe of the liver there was a circumscribed, dark red, spongy mass 4 cm in size. In the center of the mass there was a gray, firm, fibrous core.
|
(Summary of Microscopic Findings - click here)
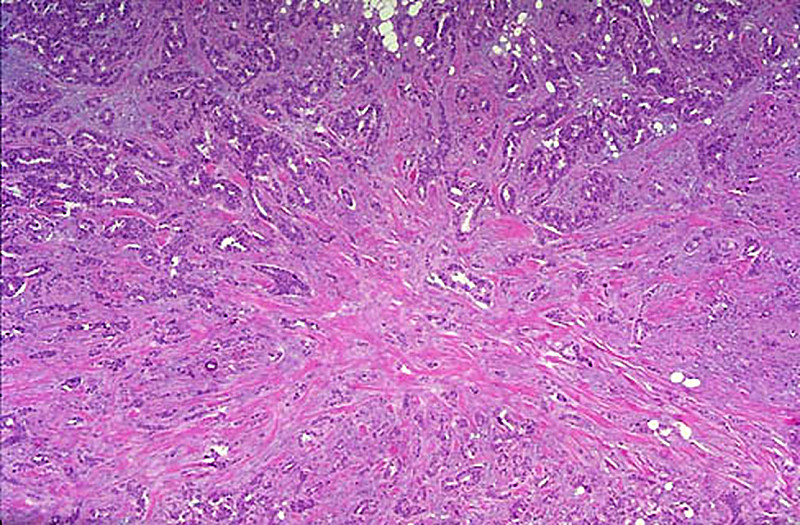
Inspection reveals a mass with many blood filled spaces. These are formed by anastomosing strands of connective tissue, partially hyalinized, lined by endothelial cells. Notice the subcapsular location of the tumor and its relationship to the liver parenchyma.
|
(Review Normal Histology - click here)
Norm No. 3 Liver
[ImageScope] [WebScope]
The liver is the organ that metabolizes nutrients received from the digestive tract. These nutrients and processed by tissue hepatocytes which are large polygonal cells. The hepatocyes are separated by portal triads. The triads consist of an artery, a vein and a bile duct. The bile duct is lined by cuboidal epithelium. The artery has a muscular wall and a flat endothelial lining. The sinuses are well defined and contain a small amount of blood.
|
|
155-1. What is the differential diagnosis?
ANSWER
155-2. Which of the following features is most suggestive of benignancy?
- Circumscription
- High mitotic rate
- Multifocal disease
- Necrosis
- Nuclear pleomorphism
ANSWER
155-3. Angiosarcoma of the liver is associated with exposure to which of the following?
- Asbestos
- Benzene
- Beryllium
- Cadmium
- Vinyl chloride
ANSWER
CASE NUMBER 170
[ImageScope] [WebScope] [DigitalScope]
Clinical History: A 67-year-old man presented to his GP with a 3-month history of weakness and fatigue. A stool guiac test was positive and colonoscopy identified a fungating 5 cm mass in his right colon. A screening CT prior to surgery is shown below. During his colectomy, the patient died due to surgical complications. At autopsy, the pathologist noticed a firm, well circumscribed mass in the lung.
Image Gallery:
(Summary of Gross Findings - click here)
A chest CT from another patient illustrating a similar "coin" lesion in the inferior lobe of the right lung is shown. There was a hard, well circumscribed, round nodule with a yellow gray cut surface in the lung.
|
(Summary of Microscopic Findings - click here)
There is normal cartilage, hyperplastic bronchial epithelium, and fragments of lung tissue with the alveoli filled with mononuclear cells derived from the alveolar epithelial cells. These lesions are common and seldom cause clinical symptoms.
|
(Review Normal Histology - click here)
Norm No. 24 Lung
[ImageScope] [WebScope]
The primary function of the lung is gas exchange. Therefore, alveoli have thin walls lined by thin flat pneumocytes and endothelial cells. There is no thickening or fibrosis of the interstitium. The bronchioli are lined with basally oriented ciliated columnar epithelium. The bronchi are lined by similar epithelium. There are mucous glands within the submucosa. The bronchial smooth muscle is not hypertrophied. The pulmonary vessels are patent with no evidence of intimal thickening or muscular hyperplasia.
|
|
170-1. What is the differential diagnosis?
ANSWER
170-2. Which of the following is the primary tissue type present in this lesion?
- Bone
- Cartilage
- Fat
- Skeletal muscle
- Smooth muscle
ANSWER
170-3. Which of the following features suggests that this is neoplastic?
- It frequently metastasizes
- It is monoclonal
- Paraneoplastic syndromes are seen
- Presence of multiple tissue types
- Over time, pleomorphism and mitotic activity increase
ANSWER
CASE NUMBER 166
[ImageScope] [WebScope] [DigitalScope]
Clinical History: A 43-year-old woman with a family history of colon cancer presented to her primary care physician with a four-month history of intermittent bloody stools. Sigmoidoscopy revealed a pedunculated polyp 15 cm from the anal sphincter. In view of her family history, she underwent a total colectomy.
Image Gallery:
(Summary of Gross Findings - click here)
The resected tissue contained several polps. The largest polyp was 1.5 cm in diameter. The stalk was 2 cm in length. The base of the stalk and the adjacent mucosa showed no induration. -
|
(Summary of Microscopic Findings - click here)
The exophytic structure of the polyp can be seen with the naked eye. There is a short stalk lined by normal colon mucosa with blood vessels in the submucosa. The finger-like villi of the polyp are lined by adenomatous mucosa, the hallmark of a neoplastic polyp. Compared to the nearby normal mucosa, the nuclei are elongated, hyperchromatic and stratified. There is increased nuclear to cytoplasmic ratio and decreased cytoplasmic mucin.
|
(Review Normal Histology - click here)
Norm No. 27 Colon
[ImageScope] [WebScope]
The colon is lined by glandular epithelium with numerous mucin secreting goblet cells. The epithelium is infolded into straight tubular glands of uniform diameter to increase the surface area available for secretion and absorption.
|
|
166-1. What is the differential diagnosis?
ANSWER
166-2. The highest risk for colon carcinoma is associated with which of the following?
- Hyperplastic polyp
- Inflammatory polyp
- Tubular adenoma.
- Tubulovillous adenoma
- Villous adenoma
ANSWER
CASE NUMBER 134
[ImageScope] [WebScope]
Clinical History: An 81-year-old asymptomatic woman was found to have guaiac-positive stool during a routine exam at her nursing home. Flexible sigmoidoscopy revealed a fungating mass and she underwent a partial colectomy.
Image Gallery:
(Summary of Gross Findings - click here)
A 4 cm fungating, centrally ulcerated mass was found on gross examination.
|
(Summary of Microscopic Findings - click here)
This section, which includes the edge of the tumor shows invasive adenocarcinoma arising in a villous adenoma. Tall villi lined by neoplastic epithelium replace the normal mucosa at the edge of the mass. Irregular glandular spaces are lined by tumor cells and large pools of mucin are seen, as well as desmoplastic (fibrotic) stroma. Although the nuclei of the carcinoma are anaplastic when compared to the normal colon mucosa, the neoplastic epithelium retains a columnar appearance, typically seen in colon carcinoma.
|
(Review Normal Histology - click here)
Norm No. 27 Colon
[ImageScope] [WebScope]
The colon is lined by glandular epithelium with numerous mucin secreting goblet cells. The epithelium is infolded into straight tubular glands of uniform diameter to increase the surface area available for secretion and absorption.
|
134-1. What is the differential diagnosis?
ANSWER
134-2. In this clinical setting, which of the following features distinguishes carcinoma from dysplasia?
- Brisk mitotic activity
- Degree of nuclear pleomorphism
- Invasion
- Presence of large nucleoli
- Ratio of dysplastic cells to normal cells
ANSWER
134-3. In colonic adenocarcinoma, which of the following is mutated earliest in the classic adenoma-carcinoma sequence?
- APC
- β catenin
- K-RAS
- p53
- Telomerase
ANSWER
134-4. Which of the following features is included in the determination of tumor stage in colonic adenocarcinoma?
- Degree of nuclear pleomorphism
- Loss of polarity
- Lymph node involvement
- Number of mitotic figures
- Surface ulceration
ANSWER
CASE NUMBER 139
[ImageScope] [WebScope] [DigitalScope]
Clinical History: During a routine physical examination, a 68-year-old man was found to have guaiac-positive stool. Colonoscopy revealed an ulcerated mass in the sigmoid colon. Laboratory analysis showed increased levels of serum alkaline phosphatase, lactate dehydrogenase and gamma glutamyltranspeptidase (GGT).
139-1. Which of the following is the most likely explanation for these laboratory findings?
- Divergent differentiation has occurred
- The patient has hepatocellular carcinoma
- The patient has an acute hepatitis C infection
- The tumor has metastasized to bone
- The tumor has metastasized to liver
ANSWER
Clinical History (continued): While in the hospital for presurgical evaluation, the patient acquired methicillin-resistant Staphylococcus aureus pneumonia and died. Gross and microscopic images from the autopsy are provided.
Image Gallery:
(Summary of Gross Findings - click here)
Large areas of the liver were replaced by a tumor masses. The tumors were firm and white in comparison to the surrounding soft, golden brown liver. Note the serrated edges of the metastases and the prominent central necrosis seen in the larger nodules. Of all neoplasms involving the liver, metastases are the most common and are usually multiple throughout the liver.
|
(Summary of Microscopic Findings - click here)
A small portion of residual liver can be seen in most sections. The tumor mass is made up of irregular glandular spaces lined by malignant, cuboidal to columnar epithelium. The neoplastic glands are dispersed in desmoplastic (fibrotic) stroma.
|
(Review Normal Histology - click here)
Norm No. 27 Colon
[ImageScope] [WebScope]
The colon is lined by glandular epithelium with numerous mucin secreting goblet cells. The epithelium is infolded into straight tubular glands of uniform diameter to increase the surface area available for secretion and absorption.
|
|
139-2. What is the differential diagnosis?
ANSWER
139-3. Which of the following is the malignancy most commonly diagnosed in the liver?
- Angiosarcoma
- Cholangiocarcinoma
- Hepatocellular carcinoma
- Hodgkin lymphoma
- Metastatic carcinoma
ANSWER
CASE NUMBER 233
[ImageScope] [WebScope]
Clinical History: A 35-year-old woman presented to her gynecologist for her first Pap test (shown below). Clinical history revealed that she had been sexually active since the age of 14 and had an abortion when she was 16. She has had no previous Pap tests. Physical exam revealed a fungating mass at the cervical os. The clinician also noted that the cervix was enlarged and felt firm. Following a biopsy, the patient underwent a hysterectomy.
Image Gallery:
(Summary of Gross Findings - click here)
The entire external cervix showed a large, gray-pink, fungating lesion, 5.5 cm in size. It extended into the internal cervical canal and also involved one of the obturator lymph nodes.
|
(Summary of Microscopic Findings - click here)
The external cervix shows fibrosis and acute and chronic inflammatory infiltration. A portion of the cervical mucosa is infiltrated with squamous cell carcinoma. The tumor cells are pleomorphic and bizarre and frequently form giant cells. Strands and nests of the tumor cells are seen in the cervical stroma. Marked acute and chronic inflammation is present in association with the tumor.
|
(Review Normal Histology - click here)
Slide 249 (cervix, H&E) WebScope ImageScope
UCSF slide 405 (cervix, trichrome) WebScope ImageScope
The uterine cervix shown in slide 249 is continuous with both the body of the uterus and the upper portion of the vagina. Note that the wall has considerable smooth muscle and much dense connective tissue. Note also the number of collagen fibers in the stroma.
The mucosa is lined by a tall columnar mucus-secreting epithelium in its uterine portion, but note the abrupt change to stratified squamous epithelium at its vaginal face. This stratocolumnar junction which should be readily identifiable in both slide 249 [example] and UCSF slide 405 [example] is frequently the site of pre-neoplastic and neoplastic (cervical cancer) changes. The mucosa is thrown into deep irregular folds known as plicae palmitae (palmate folds). During the majority of the uterine cycle these glands secrete a highly viscous mucus forming a barrier to microorganisms, while at mid-cycle (ovulation) the mucus becomes more hydrated, which facilitates sperm entry. Blockage of the openings of the cervical mucosal glands frequently results in the accumulation of secretory products within the glands, leading to the formation of dilated Nabothian cysts which may be seen in USCF slide 304 [example]. These cysts are generally benign; however, they can become clinically relevant should they become enlarged enough to cause obstruction of the cervical canal.
|
233-1. What is the differential diagnosis?
ANSWER
233-2. Which of the following is a risk factor in the development of this disease?
- Early age at menarche
- History of endocervical polyps
- Low parity
- Multiple sexual partners
- Obesity
ANSWER
233-3. Which of the following viruses is most closely associated with the development of this disease?
- HPV-1
- HPV-2
- HPV-4
- HPV-6
- HPV-11
- HPV-16
ANSWER
233-4. Which of the following is the proposed mechanism for the oncogenicity of this virus?
- CagA initiates a signaling cascade
- E7 binds RB, releasing E2F transcription factors
- LMP activates BCL2
- TAX represses CDKN2A/p16 and TP53
- Viral integration causes secondary rearrangements of chromosomes
ANSWER
CASE NUMBER 199a
[ImageScope] [WebScope]
Clinical History: A 34-year-old woman presented to her primary care physician after finding a lump in her breast during a self-exam. Physical exam revealed a 3-cm, firm, immovable mass. Mammography revealed microcalcifications. A mastectomy was performed.
Image Gallery:
(Summary of Gross Findings - click here)
There is inflammation and dimpling of the areola. The cut surface of the resected breast tissue reveals a 3 x 3 x 2 cm firm mass with stellate borders. The center of the mass is firm, scirrhous and white because of the desmoplasia. There are areas of yellowish necrosis in the portions of neoplasm infiltrating into the surrounding breast. Such tumors appear very firm and non-mobile on physical exam.
|
(Summary of Microscopic Findings - click here)
The virtual image was derived from a breast biopsy on another patient and shows both intraductal carcinoma with a comedo pattern of necrosis and invasive infiltrating ductal carcinoma. Ductal carcinomas range from well-differentiated tumors characterized by good duct formation to poorly-differentiated tumors. This one is composed of infiltrating glands and sheets of pleomorphic cells which infiltrate into the adjacent breast tissue. This infiltrating ductal carcinoma of breast at low magnification appears to radiate from a central area of desmoplasia. This collagenous component gives the neoplasm a hard "scirrhous" consistency that is palpable on physical examination or breast self-examination. Such an invasive carcinoma may be fixed to underlying chest wall, making it non-mobile. Also note the nerve which is invaded by tumor. It would also be important for treatment and prognosis to determine if the tumor cells were estrogen and progesterone receptor positive.
|
(Review Normal Histology - click here)
Norm No. 19 Female breast
[ImageScope] [WebScope]
The female breast is a secretory organ that produces milk during lactation. Breast tissue that is not stimulated to lactate consists of resting apocrine cells arranged in nests and small ductules which are lined by cuboidal epithelium. The secretory units are separated from one another by loose connective tissue.
|
199-1. What is the differential diagnosis?
ANSWER
199-2. Five years later, the patient presented with a lytic bone lesion of the right femur. A PET scan shows that the lesion is extremely avid for 18F-fluorodeoxyglucose. Which of the following features of cancer accounts for this finding?
- Epigenetic changes
- Gene amplification
- Genomic instability
- Matrix metalloproteinase activity
- Warburg effect
ANSWER
199-3. A needle biopsy of the patient’s femur lesion showed undifferentiated carcinoma. Which of the following techniques would be the next most logical step to confirm that this is metastatic breast carcinoma?
- DNA microarray analysis
- Flow cytometry
- Fluorescent in situ hybridization
- Immunohistochemistry
- Tissue culture
ANSWER
CASE NUMBER 253
[ImageScope] [WebScope]
Clinical History: A 60-year-old woman was referred to a gastroenterologist due to a one-year history of weight loss with new onset abdominal pain. Physical exam revealed occult blood present in her stool. Upper endoscopy showed a fungating, ulcerated mass in the gastric antrum and the patient underwent a partial gastrectomy.
Image Gallery:
(Summary of Gross Findings - click here)
The resected portion of the stomach showed a large fungating, partially ulcerated tumor mass in the antrum. Regional lymph nodes and a liver biopsy were free of tumor.
|
(Summary of Microscopic Findings - click here)
There is a rather abrupt change of the normal stomach mucosa to malignant tumor tissue, projecting into the lumen as a cauliflower-like mass. The tumor forms abundant irregular acini, lined by one or more layers of atypical cells with mostly large irregular nuclei and poorly defined eosinophilic cytoplasm. Atypical mitoses are moderately frequent. The tumor has infiltrated through the muscularis mucosa and the edematous submucosa and has invaded the muscle layers. The invading tumor had elicited a rather marked neutrophilic and plasma cell response.
|
(Review Normal Histology - click here)
Norm No. 16 Stomach, fundus
[ImageScope] [WebScope]
The normal gastric mucosa of the fundus contains superficial fovea arranged in leaf like fronds and deeper gastric glands. The foveolar cells secrete mucin. The gastric glands include mucous cells, parietal cells, chief cells and enteroendocrine cells.
|
253-1. What is the differential diagnosis?
ANSWER
253-2. Which of the following risk factors has the most significant association with gastric cancer?
- Alcoholism
- Cigarette smoking
- Helicobacter pylori infection
- Human papilloma virus infection
- Nitrites from nitrates in food and water
ANSWER
253-3. Germline mutations in CDH1, which encodes E-cadherin, have been identified in hereditary gastric cancer. E-cadherin plays a role in maintaining cellular adhesion and is best considered which of the following?
- DNA repair gene
- Regulator of cell cycle
- Telomerase
- Tumor oncogene
- Tumor suppressor gene
ANSWER
253-4. The link between H. pylori infection and MALT lymphoma is most closely related to which of the following?
- Altered cell surface glycolipids and glycoproteins
- Downregulation of NF-kB
- Elaboration of PTHRP by gastric epithelial cells
- MYC amplification
- Stimulation of B cells by H.pylori-reactive T cells
ANSWER
NEOPLASIA Review Items
Key Vocabulary Terms
Regarding "oncogenes" and "tumor suppressor genes:"
Oncogenes are a general class of genes that, when mutated, permit or induce uncontrolled cellular proliferation and malignant change.
Oncogenes are further classified as either protooncogenes OR tumor suppressor genes (anti-oncogenes). Protooncogenes encode proteins that stimulate DNA synthesis and cell division, including peptide growth factors and their cellular membrane receptors; second-messenger cascade proteins, which transmit information from cell membrane to nucleus; and nuclear transcription factors, which control gene expression by binding to DNA. Conversion of a protooncogene to an oncogene by amplification, translocation, or point mutation can lead to unrestrained cellular proliferation and malignant change. Only 1 copy (allele) of a protooncogene need undergo mutation to induce tumor formation. Protooncogenes are not involved in inherited cancer syndromes, with the exception of the RET protooncogene in multiple endocrine neoplasia.
Tumor suppressor genes (antioncogenes), which encode proteins that normally serve to restrain cell proliferation, can be inactivated by point mutation, deletion, or loss of expression. An inherited mutation in 1 copy of a tumor suppressor gene is the basis of most familial predispositions to cancer. Malignant cellular proliferation does not occur until the remaining, functional copy of the gene is inactivated by mutation or by deletion of part or all of its chromosome. In a person born with two normal copies of a tumor suppressor gene, both must be inactivated by mutation before tumor formation occurs. BRCA1 and BRCA2, which predispose to familial early-onset breast cancer and ovarian cancer, are tumor suppressor genes.
LEARNING OBJECTIVES
Absolutely critical information you must know to practice medicine is in bold font.
Important information that will be needed for routine patient care is in regular font.
Information about less common diseases that you may encounter in clinical practice and that will probably appear on examinations is in italics
- Compare and contrast gross, microscopic features and mode of spread:
- List the general cytologic, biochemical, antigenic, metabolic, karyotypic, and molecular genetic changes found in neoplastic cells.
- List the most common sites of origin of the following neoplasms
- Compare and contrast grading vs. staging of neoplastic disease, in terms of general principles and clinical significance
- Cite local and general mechanisms which are believed to affect the rate of tumor growth.
- Discuss how tumor growth rates are evaluated with mitotic rate and proliferation markers.
- List four major pathways by which neoplasms spread.
- Discuss metastasis of malignant neoplasms, in terms of:
- molecular genetics
- cellular adhesion
- mechanisms of invasion of extracellular matrix
- mechanisms of vascular dissemination and homing of tumor cells
- tissues and organs in which metastases are common or uncommon.
- Describe carcinogenesis, initiation, neoplastic progression and sequence of gene mutations.
- Evaluate critically the role of each of the following in the development of human cancer, general significance and at least one neoplasm associated with each:
|
|
|
|
|
|
- chronic inflammatory conditions
|
|
|
|
- Match the following agents or conditions the neoplasms with which it is related:
|
- hepatitis B and C viruses
|
|
|
|
- human papillomavirus (HPV)
|
|
- human immunodeficiency virus (HIV)
|
|
- human T cell leukemia virus type 1
|
|
|
|
|
|
|
|
|
|
|
|
|
- Discuss precancerous lesions in terms of definition, etiology, pathogenesis and growth kinetics and give common examples.
- Describe and understand the metaplasia --> dysplasia --> carcinoma-in-situ --> invasive carcinoma sequence.
- Discuss, compare, and contrast the following theories of origin of neoplasia:
|
- immune-surveillance dysfunction
|
|
|
|
|
|
|
- List the DNA viruses which have been linked to tumor formation in man and animals.
- List the connections between viruses and tumors in terms of:
- epidemiology
- interactions of virus proteins with cell regulatory proteins
- modulation of the host immune system
- Contrast the mechanisms of neoplasm formation by DNA viruses and RNA viruses.
- Discuss the relationship between protooncogenes and oncogenes, as well as the relationship between cellular oncogenes and viral oncogenes.
- Compare and contrast protooncogenes and tumor suppressor genes, in terms of genotypic vs. phenotypic expression.
- Explain the concept of recessive cancer genes.
- Describe the clinical features of following cancer-susceptibility syndromes:
- Discuss the following chromosomal translocations describing the mechanism of oncogenesis and associated neoplasms:
- Discuss chemical carcinogenesis in terms of dose dependency.
- Explain the carcinogenic effect of irradiation.
- Cite evidence for estrogens as carcinogens.
- Describe the body's immune system and its role in the development of neoplasms including anti-tumor immunity and immunologic surveillance
- Discuss the different types of escape mechanisms utilized by neoplasms to evade the immunosurveillance system of an immunocompetent host.
- Discuss tumor specific antigens and tumor related antigens, in terms of:
- importance in anti-tumor immunity
- Compare and contrast tumors transmitted by dominant inheritance and recessive inheritance. Give examples of each.
- Compare and contrast acquired cancer-causing genetic mutations and germline cancer-causing genetic mutations. Give examples of each.
- Describe the indications, advantages, and disadvantages of diagnostic procedures and laboratory tests used to diagnose, and monitor the progression of neoplasms:
|
|
|
|
- magnetic resonance imaging (MRI)
|
|
|
|
|
- fine needle aspiration (FNA) cytology
|
- positron emission tomography (PET)
|
|
|
|
|
|
-
List the secretions or other fluids examined by cytology for diagnosis of malignancy.
-
List the organs in which cytology plays an important role in cancer case findings.
- For both males and females, list in descending order:
- five most common causes of cancer death
- List the relative incidence and mortality of cancer for each sex and decade of age.
- Discuss the mechanism by which neoplasms produce each of the following, listing neoplasms that are commonly associated with each effect:
- Match each of the following public health measures with neoplasms in which it may be used.
|
|
- avoidance of ionizing radiation
|
|
- avoidance of excessive sunlight
|
- routine laboratory studies
|
|
- routine physical examination
|
|
|
- Match each of these tumor markers with the neoplasm(s) with which it is associated:
- human chorionic gonadotrophin (HCG)
- calcitonin
- catecholamines
- α-fetoprotein (AFP)
- Contrast the effects of benign and malignant tumors on the host.
- List the common signs and symptoms of malignancy.
- List the common causes of death from cancer.
LABORATORY MEDICINE Review Items
Key Vocabulary Terms
LEARNING OBJECTIVES
- Describe the activities of clinical pathologists, (laboratory medicine).
- Describe the appropriate uses of clinical laboratories.
- Calculate sensitivity and specificity from a 2 X 2 table.
- Compare and contrast precision and accuracy.
- Discuss development of "normal range", including reference group method, prognosis/treatment derived, threshold value, and therapeutic drug reference range.
- Compare and contrast preanalytical, analytical, and postanalytical variables in laboratory testing, and give examples of each.
- Discuss the effects of sample handling on laboratory results, including turnaround time, type of tube used for blood collection, timing of collection, transport, and storage.
|