Case assignments by lab group and class day:
CASE NUMBER 221
(no virtual slide for this case)
Clinical History: A 55-year-old man underwent total nephrectomy for renal cell carcinoma and subsequently received adjuvant chemotherapy. While on chemotherapy, he became leukopenic and thrombocytopenic. He presented to his oncologist with a 3-day history of a rash on his left side.
221-1. What is the differential diagnosis?
ANSWER
Image Gallery:
(Summary of Gross Findings)
There is a band-like papulovesicular rash with lesions averaging 3-5 mm in size.
|
(Summary of Microscopic Findings)
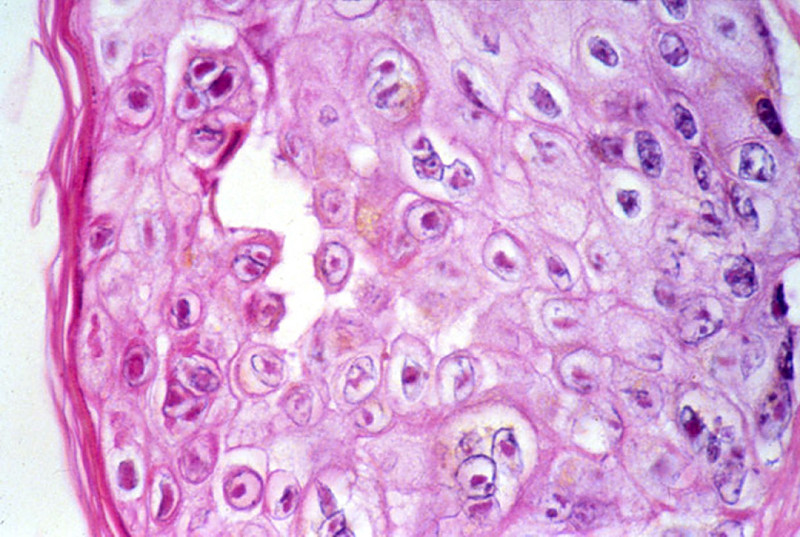
The epidermis shows spongiosis, vesicle formation, necrosis and ulceration. The epidermal cells have degrees of ballooning degeneration. Many intranuclear eosinophilic inclusion bodies are seen in these cells. Many keratinocytes within the vesicle also have multiple nuclei with nuclear "molding" and marginated chromatin. The upper dermis beneath a vesicle shows necrosis with little or no inflammatory reaction.
|
221-2. Which of the following is the etiologic agent for this disease?
- Cytomegalovirus
- Herpes simplex virus-2
- Human papilloma virus, type 6
- Poliovirus
- Varicella-zoster virus
ANSWER
221-3. Where is latent infection established following primary infection?
- Dorsal root ganglia
- Motor axons
- Neuromuscular junction
- Peripheral sensory nerves
- Skeletal muscle
ANSWER
221-4. Which of the following is a rare complication that can be seen in this disease?
- B-cell lymphoma
- Facial hemiparesis
- Myocarditis
- Toxic shock syndrome
- Vegetations on heart valves
ANSWER
CASE NUMBER 544
(no virtual slide for this case)
Clinical History: A 5-year-old boy is brought to the pediatrician because his parents notice that he walks on his toes and has difficulty climbing stairs. They state that he did not begin walking until he was 18 months old. Physical exam reveals bilaterally enlarged calves. A muscle biopsy is performed.
544-1. What is the differential diagnosis?
ANSWER
Image Gallery:
| |
(Summary of Microscopic Findings)
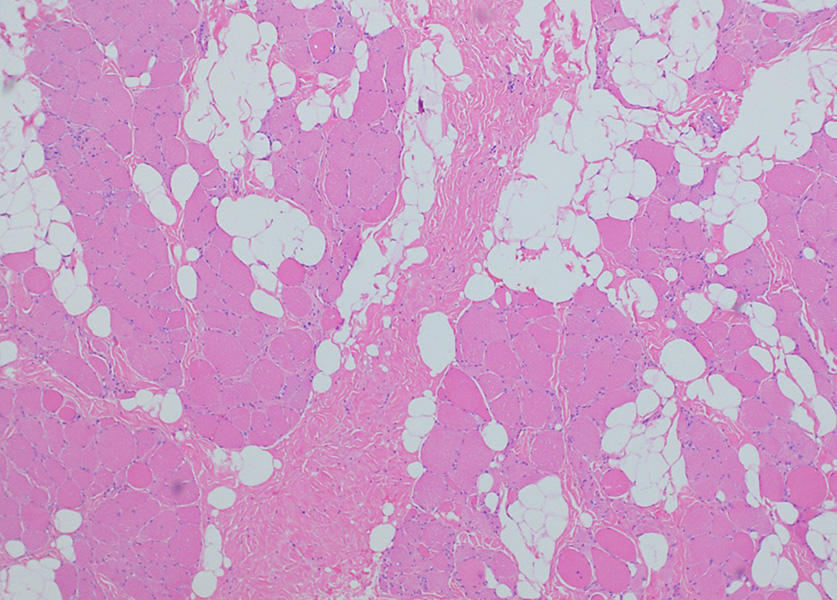
The low power view (left) shows fatty replacement of muscle fibers and hypertrophy and atrophy of fibers. The higher power view (right) shows marked fibrosis, fiber splitting, degeneration/myophagocytosis, and regeneration (internal nuclei).
|
Clinical History, part 2 (click here when instructed)
CASE NUMBER 523- slide courtesy of UMich
[ImageScope] [WebScope]
Clinical History: An 18-year-old man presents for his Army physical. The doctor notices multiple skin lesions distributed evenly across his body and irregular areas of hyperpigmentation. The patient states that he has had these lesions his entire life but that they had never bothered him. One of the lesions is biopsied.
523-1. What is the differential diagnosis?
ANSWER
Image Gallery:
(Summary of Clinical Findings)
There are multiple soft, fleshy, pedunculated lesions present. In addition, there is a focus of hyperpigmentation consistent with a café au lait spot.
|
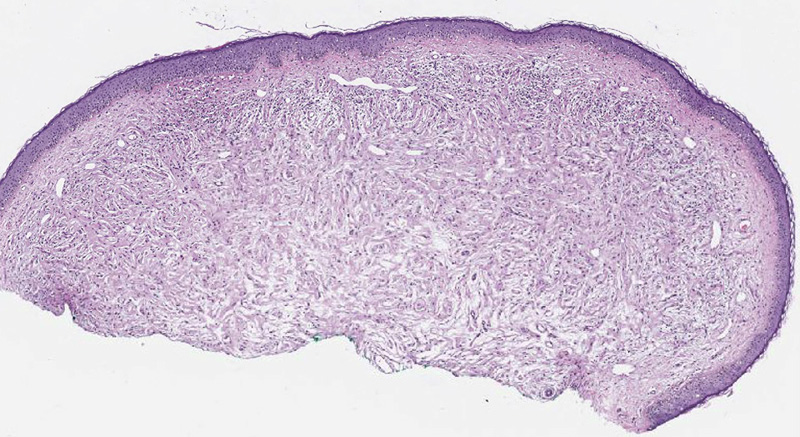
(Summary of Microscopic Findings)
There is an infiltrative, non-circumscribed lesion present in the dermis that is composed of wavy or buckled spindle cells distributed amidst ropy collagen bundles and myxoid stroma. Mitotic activity, necrosis and cryptologic atypia are not seen.
|
Cerebrum
Slide 76 (cerebrum, luxol blue/cresyl violet) [WebScope] [ImageScope]
Slide 76b (toluidine blue & eosin) [WebScope] [ImageScope]
The cerebral cortex is loosely stratified into layers containing scattered nuclei of both neurons and glial cells. Examine the layered organization of the cerebral cortex using slide 76 stained with luxol blue/cresyl violet [ORIENTATION] (which stains white matter tracts and cell bodies) or toluidine blue and eosin [ORIENTATION] (TB&E, toluidine blue stains the nuclei and RER of cells whereas eosin stains membranes and axon tracts). Typically one or more sulci (infoldings) will extend inward from one edge of the section. Examine the gray matter on each side of the sulcus using first low and then high power. Neurons of the cerebral cortex are of varying shapes and sizes, but the most obvious are pyramidal cells. As the name implies, the cell body is shaped somewhat like a pyramid, with a large, branching dendrite extending from the apex of the pyramid toward the cortical surface, and with an axon extending downward from the base of the pyramid. In addition to pyramidal cells, other nuclei seen in these sections may belong to other neurons or to glial cells also present in the cortex. You may be able to see subtle differences in the distribution of cell types in rather loosely demarcated layers. There are 6 classically recognized layers of the cortex:
- Outer plexiform (molecular) layer: sparse neurons and glia
- Outer granular layer: small pyramidal and stellate neurons
- Outer pyramidal layer: moderate sized pyramidal neurons (should be able to see these in either luxol blue [example] or TB&E-stained [example] sections)
- Inner granular layer: densely packed stellate neurons (usually the numerous processes aren’t visible, but there are lots of nuclei reflecting the cell density)
- Ganglionic or inner pyramidal layer: large pyramidal neurons (should be able to see these in either luxol blue [example] or TB&E-stained [example] sections)
- Multiform cell layer: mixture of small pyramidal and stellate neurons
Pyramidal cells in layers III and V tend to be larger because their axons contribute to efferent projections that extend to other regions of the CNS –pyramidal neurons in layer V of motor cortices send projections all the way down to motor neurons in the spinal cord!
Deep to the gray matter of the cerebral cortex is the white matter that conveys myelinated fibers between different parts of the cortex and other regions of the CNS. Be sure you identify the white matter in both luxol blue [example] and TB&E-stained [example] sections, as it will appear differently in these two stains. Review the organization of gray and white matter in cerebral cortex vs. spinal cord.
|
523-2. A mutation in a gene encoding which of the following is most commonly observed in patients with this disease?
- Dystrophin
- E-cadherin
- Merlin
- Neurofibromin
- Tuberin
ANSWER
523-3. Identification of which of the following is highly suggestive of this diagnosis?
- Hemangioblastoma
- Meningioma
- Plexiform neurofibroma
- Solitary cutaneous neurofibroma
- Vestibular schwannoma
ANSWER
Clinical History (continued): Ten years later, the patient presents to his primary care physician with a 3-week history of “burning” and “shooting” nerve pain in his right arm. MRI revealed a 5 cm mass within the brachial plexus. The mass was excised.
523-4. What is the differential diagnosis?
ANSWER
Image Gallery:
[ImageScope] [WebScope] - slide courtesy of UMich
<(Summary of Microscopic Findings)
Residual neurofibroma is present on the superior aspect of the tissue. The remaining tissue shows fascicular architecture, cytologic atypia, hypercellularity and scattered mitotic figures. There is focal necrosis and vascular invasion.
|
523-5. Which of the following is the life time risk for developing this type of tumor in a patient with this disease?
- <1%
- 1 – 10%
- 21 - 30%
- 51 - 60%
- >90%
ANSWER
CASE NUMBER 390- slide courtesy of UMich
[ImageScope] [WebScope]
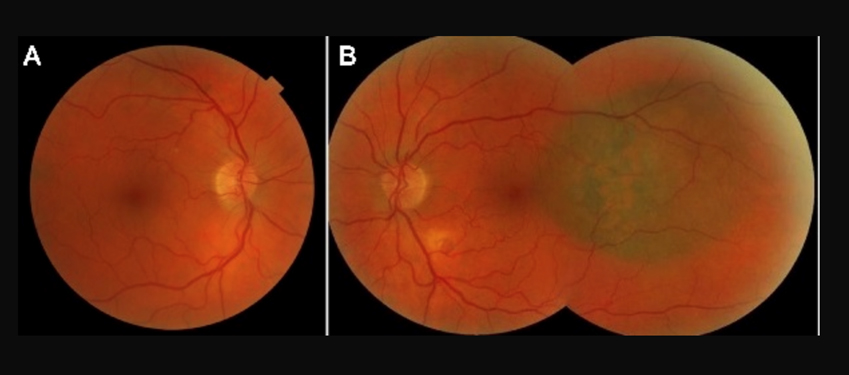
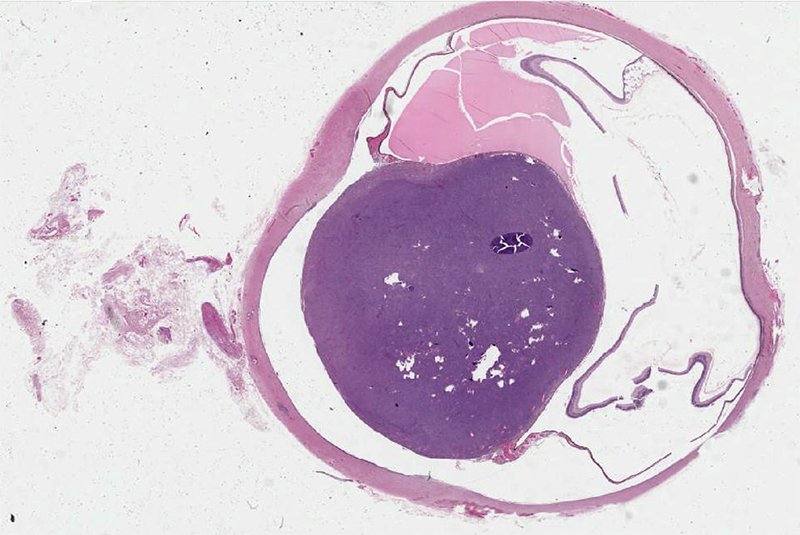
Clinical History:A 58-year-old man presented to his primary care physician with a 3-month history of blurred vision in his left eye. Previously, he had 20-20 vision in both eyes and had not seen an ophthalmologist since he was in college.
A fundoscopic exam revealed a pigmented lesion near the fovea. (A) Right eye (B) left eye. Ultrasonographic examination confirmed a diameter of 10 mm with a thickness of 2.5 mm.
390-1. What is the differential diagnosis?
ANSWER
Image Gallery:
(Summary of Clinical Findings)
There are multiple soft, fleshy, pedunculated lesions present. In addition, there is a focus of hyperpigmentation consistent with a café au lait spot.
|
(Summary of Microscopic Findings)
There is an infiltrative, non-circumscribed lesion present in the dermis that is composed of wavy or buckled spindle cells distributed amidst ropy collagen bundles and myxoid stroma. Mitotic activity, necrosis and cryptologic atypia are not seen.
|
Cerebrum
Slide 76 (cerebrum, luxol blue/cresyl violet) [WebScope] [ImageScope]
Slide 76b (toluidine blue & eosin) [WebScope] [ImageScope]
The cerebral cortex is loosely stratified into layers containing scattered nuclei of both neurons and glial cells. Examine the layered organization of the cerebral cortex using slide 76 stained with luxol blue/cresyl violet [ORIENTATION] (which stains white matter tracts and cell bodies) or toluidine blue and eosin [ORIENTATION] (TB&E, toluidine blue stains the nuclei and RER of cells whereas eosin stains membranes and axon tracts). Typically one or more sulci (infoldings) will extend inward from one edge of the section. Examine the gray matter on each side of the sulcus using first low and then high power. Neurons of the cerebral cortex are of varying shapes and sizes, but the most obvious are pyramidal cells. As the name implies, the cell body is shaped somewhat like a pyramid, with a large, branching dendrite extending from the apex of the pyramid toward the cortical surface, and with an axon extending downward from the base of the pyramid. In addition to pyramidal cells, other nuclei seen in these sections may belong to other neurons or to glial cells also present in the cortex. You may be able to see subtle differences in the distribution of cell types in rather loosely demarcated layers. There are 6 classically recognized layers of the cortex:
- Outer plexiform (molecular) layer: sparse neurons and glia
- Outer granular layer: small pyramidal and stellate neurons
- Outer pyramidal layer: moderate sized pyramidal neurons (should be able to see these in either luxol blue [example] or TB&E-stained [example] sections)
- Inner granular layer: densely packed stellate neurons (usually the numerous processes aren’t visible, but there are lots of nuclei reflecting the cell density)
- Ganglionic or inner pyramidal layer: large pyramidal neurons (should be able to see these in either luxol blue [example] or TB&E-stained [example] sections)
- Multiform cell layer: mixture of small pyramidal and stellate neurons
Pyramidal cells in layers III and V tend to be larger because their axons contribute to efferent projections that extend to other regions of the CNS –pyramidal neurons in layer V of motor cortices send projections all the way down to motor neurons in the spinal cord!
Deep to the gray matter of the cerebral cortex is the white matter that conveys myelinated fibers between different parts of the cortex and other regions of the CNS. Be sure you identify the white matter in both luxol blue [example] and TB&E-stained [example] sections, as it will appear differently in these two stains. Review the organization of gray and white matter in cerebral cortex vs. spinal cord.
|
390-2. Which oncogene is most commonly mutated in this disease?
- BAP1
- CFH
- GNAQ
- RHO
- USH2A
ANSWER
390-3. Which feature is associated with worse prognosis in this disease?
- Depth of invasion
- Lateral extent of tumor
- Origination in the iris
- Spindle cell morphology
- Ulceration
ANSWER
390-4. Which of the following is the most common site of metastasis for this tumor?
- Bone
- Brain
- Liver
- Lung
- Soft tissue
ANSWER
MUSCLE PATHOLOGY Review Items
Muscle Pathology Key Vocabulary Terms (click here to search any additional terms on Stedman's Online Medical Dictionary)
Eye Pathology Key Vocabulary Terms (click here to search any additional terms on Stedman's Online Medical Dictionary)
PNS: GOALS and LEARNING OBJECTIVES
Goal: Neuromuscular and Muscular Disorders
Apply knowledge of clinical, anatomic and neuropathologic principles to the diagnosis of neuromuscular and muscular disorders.
- Objective 1: Amyotrophic Lateral Sclerosis
Describe the etiology, pathogenesis, and clinical features of amyotrophic lateral sclerosis.
- Objective 2: Mitochondrial Disorders
Describe the etiology, pathogenesis, and clinical features of mitochondrial diseases affecting muscle.
- Objective 3: Muscular Dystrophies
Compare and contrast the etiology, pathogenesis, and clinical features of the dystrophiopathies.
- Objective 4: Acquired Disorders of Skeletal Muscle
Compare and contrast the etiology, pathogenesis, and clinical features of inflammatory myopathies and toxic myopathies.
Goal: Pathology of Peripheral Nerves
Apply knowledge of clinical, anatomic and neuropathologic principles to the diagnosis of neural disorders.
- Objective 1: Disorders Associated with Peripheral Nerve Injury
Compare and contrast the peripheral neuropathies in terms of etiology, risk factors, clinical presentation, pathologic findings and natural history.
- Objective 2: Disorders of the Neuromuscular Junction
Compare and contrast the disorders of the neuromuscular junction in terms of etiology, risk factors, clinical presentation, pathologic findings and natural history.
- Objective 3: Peripheral Nerve Sheath Tumors
Compare and contrast benign and malignant tumors of the peripheral nerve sheath in terms of etiology, genetics, associated syndromes, clinical presentation, pathologic findings and prognostic factors.
|