CASE NUMBER 370 - slide courtesy of UMich
[ImageScope] [WebScope]
Clinical History: A 67-year-old woman with a long history of hypertension and a remote myocardial infarction presented to the emergency department with a two-hour history of left-sided weakness. She reported that she had a “fluttering” sensation in her chest and that her cardiologist had recommended treatment for atrial fibrillation which she had refused. While in the emergency department, she developed left-sided hemiparesis. She was admitted to the hospital for observation; however, her condition worsened and she went into a coma. She died 17 days after admission.
Image Gallery:
(Summary of Gross Findings - click here)
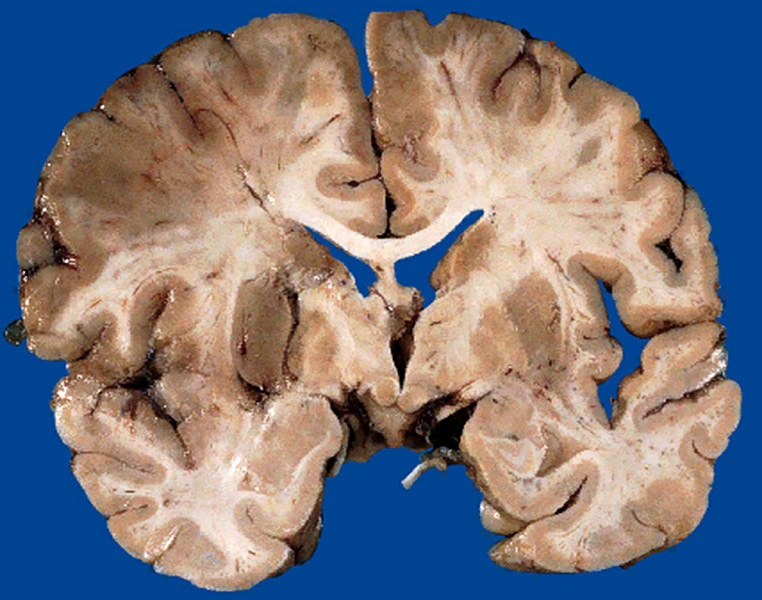
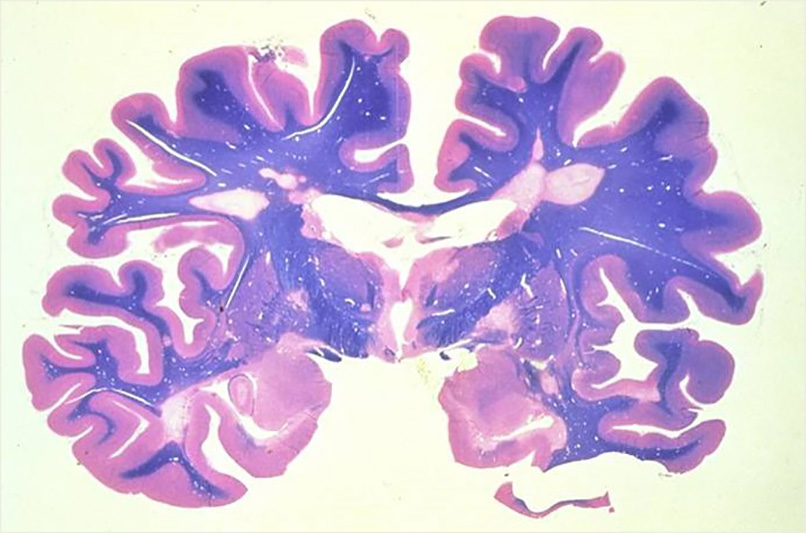
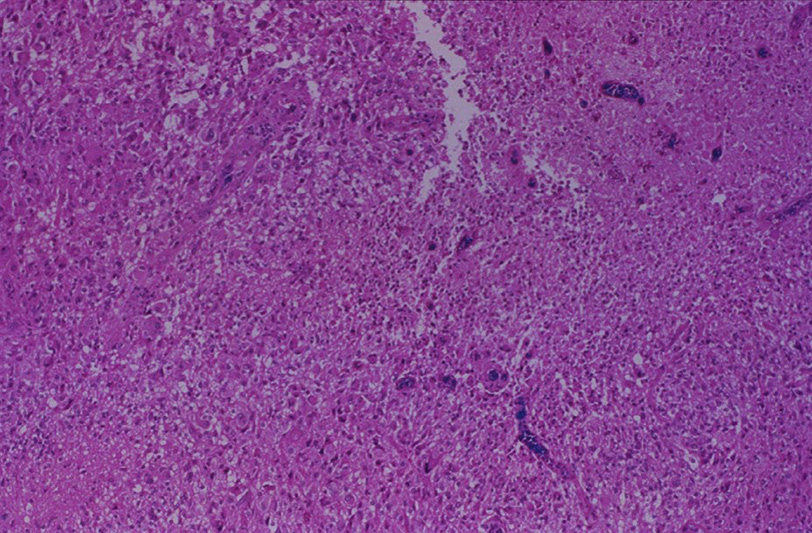
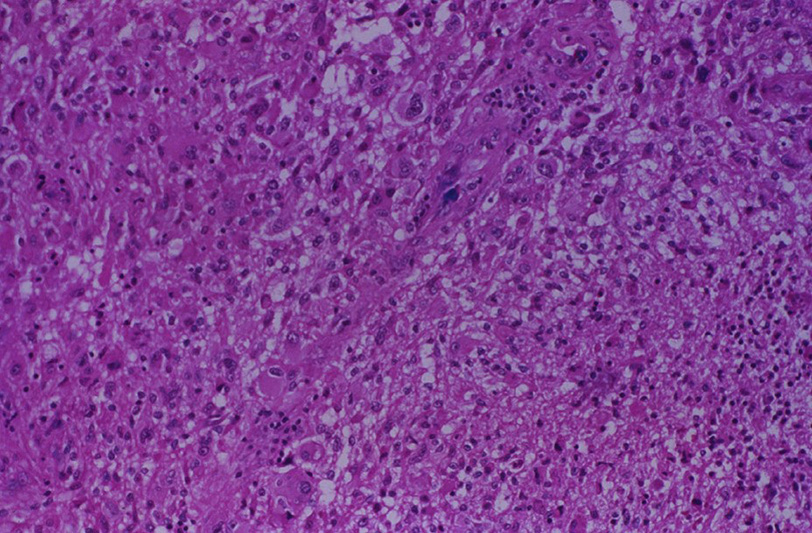
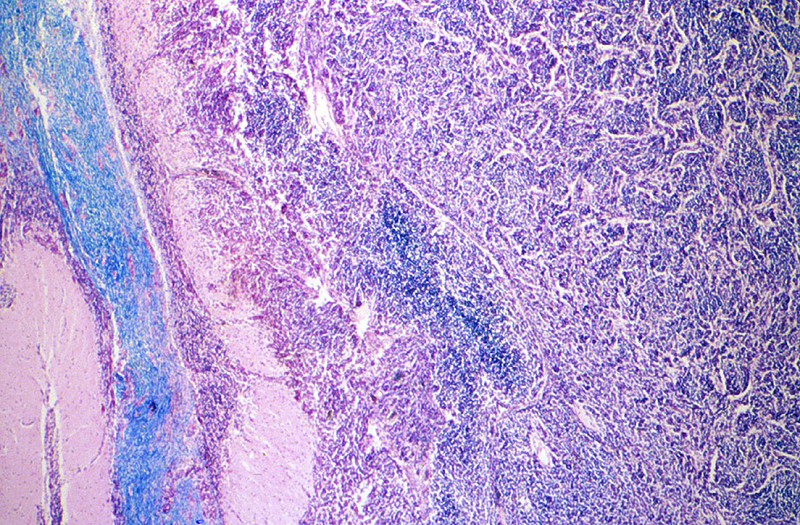
There was thrombosis of the right internal carotid artery just above the bifurcation. There was extensive necrosis of the right frontal, parietal and temporal lobes and basal ganglia.
|
(Summary of Microscopic Findings - click here)
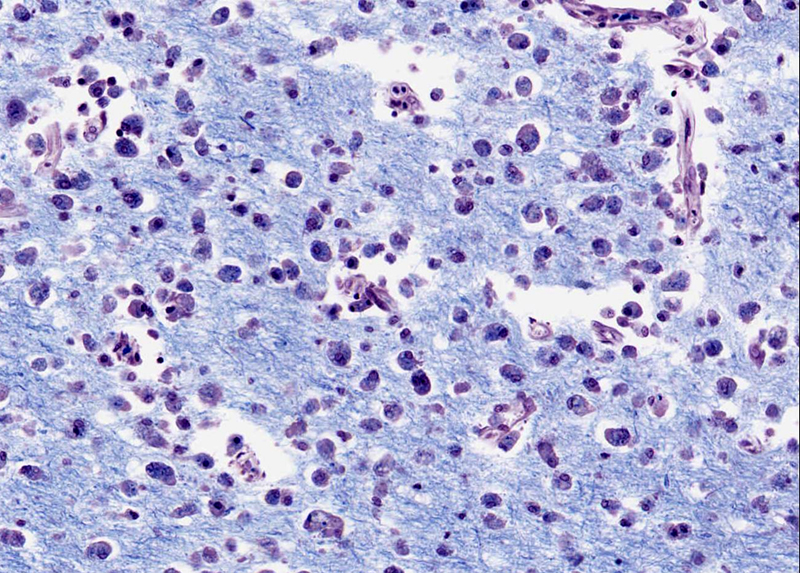
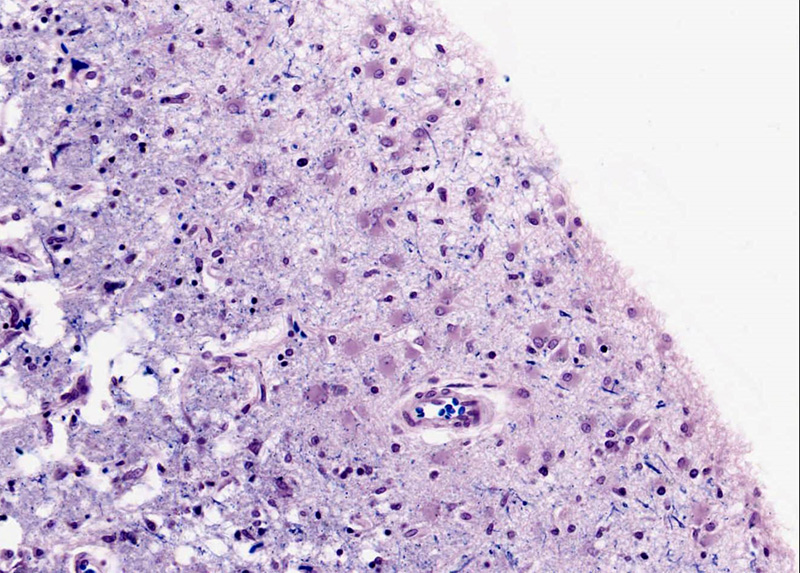
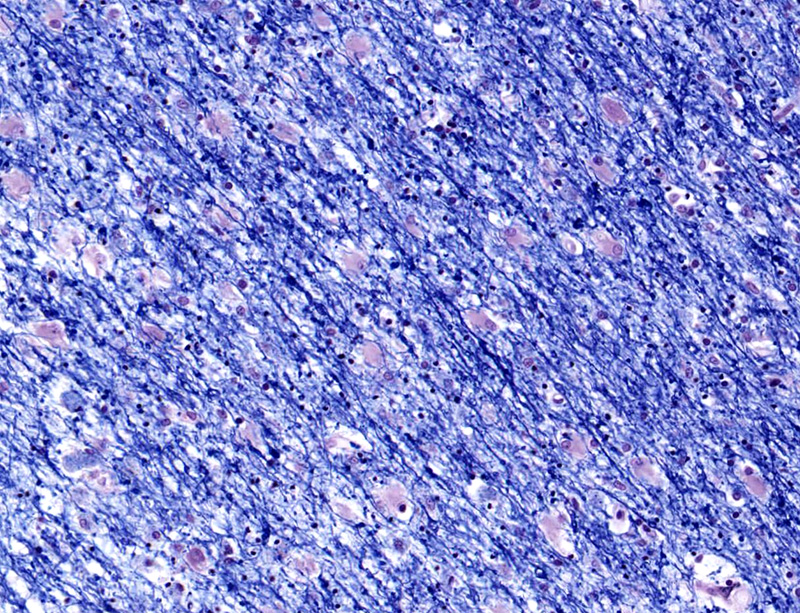
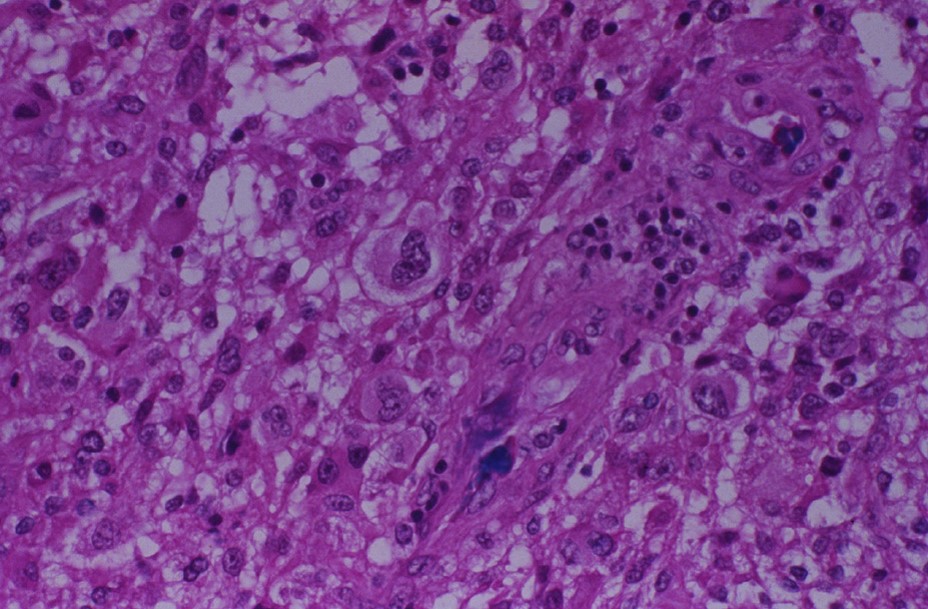
This is a luxol stain, which stains cell bodies (most abundant in the cortex) light pink whereas myelin (most abundant in the white matter) is dark blue. There is an area of liquefactive necrosis in which many macrophages with phagocytosed fat and myelin particles are present. At the pial surface and within the white matter surrounding the necrotic area are numerous large astrocytes (reactive gliosis) with large vesicular nuclei and abundant eosinophilic cytoplasm. The myelin in this area stains pale (compared to more healthy white matter seen on the right side of the slide) due to surrounding edema fluid. The blood vessels are congested and there is some extravasated blood. (H&E stain)
|
(Review Normal Histology - click here)
Cerebrum
Slide 76 (cerebrum, luxol blue/cresyl violet) [WebScope] [ImageScope]
Slide 76b (toluidine blue & eosin) [WebScope] [ImageScope]
The cerebral cortex is loosely stratified into layers containing scattered nuclei of both neurons and glial cells. Examine the layered organization of the cerebral cortex using slide 76 stained with luxol blue/cresyl violet [ORIENTATION] (which stains white matter tracts and cell bodies) or toluidine blue and eosin [ORIENTATION] (TB&E, toluidine blue stains the nuclei and RER of cells whereas eosin stains membranes and axon tracts). Typically one or more sulci (infoldings) will extend inward from one edge of the section. Examine the gray matter on each side of the sulcus using first low and then high power. Neurons of the cerebral cortex are of varying shapes and sizes, but the most obvious are pyramidal cells. As the name implies, the cell body is shaped somewhat like a pyramid, with a large, branching dendrite extending from the apex of the pyramid toward the cortical surface, and with an axon extending downward from the base of the pyramid. In addition to pyramidal cells, other nuclei seen in these sections may belong to other neurons or to glial cells also present in the cortex. You may be able to see subtle differences in the distribution of cell types in rather loosely demarcated layers. There are 6 classically recognized layers of the cortex:
- Outer plexiform (molecular) layer: sparse neurons and glia
- Outer granular layer: small pyramidal and stellate neurons
- Outer pyramidal layer: moderate sized pyramidal neurons (should be able to see these in either luxol blue [example] or TB&E-stained [example] sections)
- Inner granular layer: densely packed stellate neurons (usually the numerous processes aren’t visible, but there are lots of nuclei reflecting the cell density)
- Ganglionic or inner pyramidal layer: large pyramidal neurons (should be able to see these in either luxol blue [example] or TB&E-stained [example] sections)
- Multiform cell layer: mixture of small pyramidal and stellate neurons
Pyramidal cells in layers III and V tend to be larger because their axons contribute to efferent projections that extend to other regions of the CNS –pyramidal neurons in layer V of motor cortices send projections all the way down to motor neurons in the spinal cord!
Deep to the gray matter of the cerebral cortex is the white matter that conveys myelinated fibers between different parts of the cortex and other regions of the CNS. Be sure you identify the white matter in both luxol blue [example] and TB&E-stained [example] sections, as it will appear differently in these two stains. Review the organization of gray and white matter in cerebral cortex vs. spinal cord.
|
370-1. Which of the following is the most likely diagnosis?
- Acute meningitis
- Brain infarct
- Diffuse axonal injury
- Intracranial hemorrhage
- Ruptured saccular aneurysm
370-2. Which of the following is the cause of the majority of thrombotic occlusions?
- Atherosclerosis
- Bacterial endocarditis
- Bone marrow embolization
- Infectious vasculitis
- Polyarteritis nodosa
370-3. Which of the following microscopic features is seen in the brain 12 to 24 hours after an acute hypoxic event?
- Abundant phagocytic cells
- Central chromatolysis
- Cystic change
- Reactive astrocytosis
- Red neurons
370-4. Which of the following mechanisms explains the connection between atrial fibrillation and brain infarction?
- Association with Libman-Sacks disease
- Deformation of red blood cells causes vascular occlusions
- Increased incidence of nonbacterial thrombotic endocarditis
- Mural thrombi due to non-laminar flow
- Intracranial vasospasm due to decreased oxygenation
CASE NUMBER 504
(no virtual slide for this case)
Clinical History: A 25-year-old woman presented to her primary care physician with a one-week history of blurred vision in her left eye. She stated that it was painful to move that eye. She grew up in Minnesota and has smoked one-half of a pack of cigarettes/day for the last 7 years. Further questioning reveals that she had unilateral tingling on her left side in the two weeks before her wedding 3 years ago. CSF analysis showed mildly elevated protein and moderate pleocytosis. MRI revealed multiple hypointense lesions and FLAIR (fluid-attenuated inversion recovery) MRI showed multiple supratentorial lesions. When the patient learned of her possible diagnosis, she returned home and took an overdose of sleeping pills.
Image Gallery:
504-1. Which of the following is the most likely diagnosis?
- Alzheimer disease
- Amyotrophic lateral sclerosis
- Huntington disease
- Multiple sclerosis
- Multiple system atrophy
504-2. The lesions in this disease are caused by an immune response directed against which of the following?
- Amyloid precursor protein
- Aquaporins
- Huntingtin
- Myelin sheath
- Substantia nigra
CASE NUMBER 427
[ImageScope] [WebScope]
Clinical History: A 78-year-old man presented to his primary care physician with a two-year history of headache that had worsened recently. In addition, he said that he had difficulty seeing. Visual field examination revealed bitemporal hemianopsia. No endocrine abnormalities were identified. He was admitted to the hospital for evaluation where MRI showed a 1.5 cm suprasellar mass. Screening CT showed no other abnormalities. While in the hospital, the patient contracted pneumonia and died. No other CNS pathology was noted at autopsy.
Image Gallery:
(Summary of Gross Findings - click here)
The pituitary gland, weighing 3 gms and measuring 2 cms in greatest diameter, contained a large pink-gray soft tumor mass in the anterior lobe. The optic chiasm was slightly atrophic due to the compression of the tumor.
|
(Summary of Microscopic Findings - click here)
The tumor occupies nearly the entire anterior lobe, so that only a thin rim of normal hypophyseal tissue is present in the subcapsular area. The tumor is composed of uniform cells arranged in a trabecular or sinusoidal pattern. The stroma is highly vascular. Some of the tumor cells contain fine eosinophilic granules, but most of them are chromophobes with special stains.
|
(Review Normal Histology - click here)
Cerebrum
Slide 76 (cerebrum, luxol blue/cresyl violet) [WebScope] [ImageScope]
Slide 76b (toluidine blue & eosin) [WebScope] [ImageScope]
The cerebral cortex is loosely stratified into layers containing scattered nuclei of both neurons and glial cells. Examine the layered organization of the cerebral cortex using slide 76 stained with luxol blue/cresyl violet [ORIENTATION] (which stains white matter tracts and cell bodies) or toluidine blue and eosin [ORIENTATION] (TB&E, toluidine blue stains the nuclei and RER of cells whereas eosin stains membranes and axon tracts). Typically one or more sulci (infoldings) will extend inward from one edge of the section. Examine the gray matter on each side of the sulcus using first low and then high power. Neurons of the cerebral cortex are of varying shapes and sizes, but the most obvious are pyramidal cells. As the name implies, the cell body is shaped somewhat like a pyramid, with a large, branching dendrite extending from the apex of the pyramid toward the cortical surface, and with an axon extending downward from the base of the pyramid. In addition to pyramidal cells, other nuclei seen in these sections may belong to other neurons or to glial cells also present in the cortex. You may be able to see subtle differences in the distribution of cell types in rather loosely demarcated layers. There are 6 classically recognized layers of the cortex:
- Outer plexiform (molecular) layer: sparse neurons and glia
- Outer granular layer: small pyramidal and stellate neurons
- Outer pyramidal layer: moderate sized pyramidal neurons (should be able to see these in either luxol blue [example] or TB&E-stained [example] sections)
- Inner granular layer: densely packed stellate neurons (usually the numerous processes aren’t visible, but there are lots of nuclei reflecting the cell density)
- Ganglionic or inner pyramidal layer: large pyramidal neurons (should be able to see these in either luxol blue [example] or TB&E-stained [example] sections)
- Multiform cell layer: mixture of small pyramidal and stellate neurons
Pyramidal cells in layers III and V tend to be larger because their axons contribute to efferent projections that extend to other regions of the CNS –pyramidal neurons in layer V of motor cortices send projections all the way down to motor neurons in the spinal cord!
Deep to the gray matter of the cerebral cortex is the white matter that conveys myelinated fibers between different parts of the cortex and other regions of the CNS. Be sure you identify the white matter in both luxol blue [example] and TB&E-stained [example] sections, as it will appear differently in these two stains. Review the organization of gray and white matter in cerebral cortex vs. spinal cord.
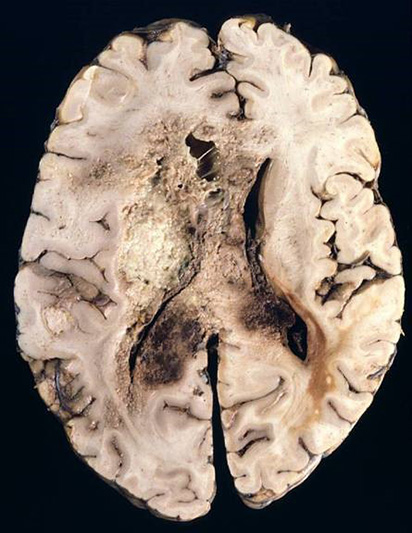
This section of brain is stained with hematoxylin and eosin. The tumor of the left side of the brain was due to the proliferation and infiltration of moderately pleomorphic fibrillary astrocytic cells. There is focal necrosis. Necrosis is the hallmark of glioblastoma. Better differentiated slower growing astrocytomas do not exhibit necrosis. |
427-1. Which of the following is the most likely diagnosis?
- Craniopharyngioma
- Meningioma
- Metastatic renal cell carcinoma
- Pituitary adenoma
- Pituitary carcinoma
427-2. Which of the following is true regarding pituitary adenoma?
- Classification is based on size and location
- It can be distinguished from hyperplasia by its pleomorphism and well-formed reticulin network
- G-protein mutations are commonly seen in somatotroph cell adenomas
- Gonadotroph adenomas cause Cushing syndrome
- Malignant transformation occurs in 25% of cases
CASE NUMBER 221
(no virtual slide for this case)
Clinical History: A 62-year-old white man underwent total nephrectomy for renal cell carcinoma and subsequently received adjuvant chemotherapy. While on chemotherapy, he became leukopenic and thrombocytopenic. He presented to his oncologist with a 3-day history of a rash on his right shoulder.
Image Gallery:
(Summary of Gross Findings - click here)
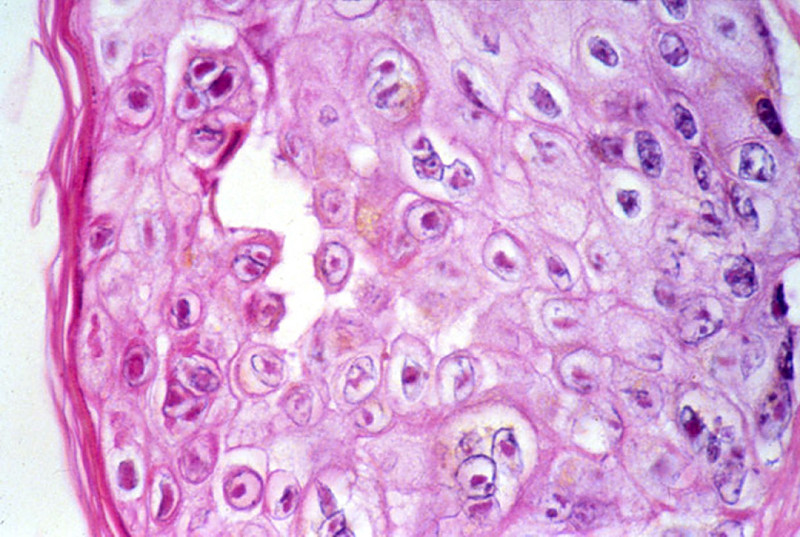
There is a linear papulovesicular rash with lesions averaging 3-5 mm in size.
|
(Summary of Microscopic Findings - click here)
The epidermis shows spongiosis, vesicle formation, necrosis and ulceration. The epidermal cells have degrees of ballooning degeneration. Many intranuclear eosinophilic inclusion bodies are seen in these cells. Many keratinocytes within the vesicle also have multiple nuclei with nuclear "molding" and marginated chromatin. The upper dermis beneath a vesicle shows necrosis with little or no inflammatory reaction.
|
221-1. Which of the following is the most likely diagnosis?
- Bullous pemphigoid
- Dermatitis herpetiformis
- Epidermolysis bullosa
- Erythema multiforme
- Shingles
221-2. Which of the following is involved in the pathogenesis of this disease?
- IgA antibodies to gluten cross-react with reticulin
- Infection with Varicella-Zoster virus
- Keratinocyte destruction by cytotoxic T cells
- Linear deposits of IgG and complement at the dermoepidermal junction
- Mutation in the type VII collagen gene
221-3. Which of the following is a rare outcome that can be seen in this disease?
- B-cell lymphoma
- Facial hemiparalysis
- Myocarditis
- Toxic shock syndrome
- Vegetations on heart valves
CASE NUMBER 503
(no virtual slide for this case)
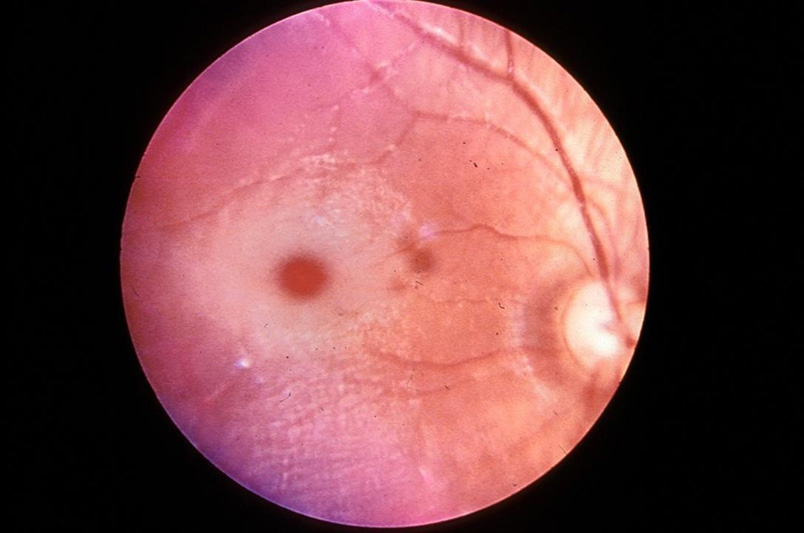
Clinical History: A mother brought her 3-month-old infant to the pediatrician because the child had been alternately crying inconsolably or lying down listlessly; vomiting for the last 3 days, and had a mild fever. Physical exam reveals cherry red maculas. CSF analysis shows elevated protein levels. Gene sequencing reveals a mutation in the a-subunit of hexosaminidase A.
Image Gallery:
503-1. Which of the following is the most likely diagnosis?
- Fabry disease
- Gaucher disease
- Krabbe disease
- Metachromatic leukodystrophy
- Tay-Sachs disease
503-2. This disease is classified as which of the following?
- Glycogenosis
- Mucopolylipidosis
- Mucopolysaccharidosis
- Sphingolipidosis
- Sulfatidosis
503-3. Which of the following is true regarding this disease?
- Boys are affected more commonly than girls
- Most patients recover full neurological function in their teens
- The “cherry red macula” is due to retinal hemangiomas
- There is an increased incidence in Ashknazi Jews
- These patients are at increased risk for colon cancer
CASE NUMBER 327
(no virtual slide for this case)
Clinical History: A 46-year-old man presented to his primary care physician with a three-week history of weakness of the right arm and leg and difficulty speaking. MRI revealed a large tumor in the left parietal lobe. Following a biopsy, the patient was treated with chemotherapy and radiation therapy because the tumor was unresectable. He died one year after diagnosis.
Image Gallery:
327-1. Which of the following is the most likely diagnosis?
- Astrocytoma
- Ependymoblastoma
- Glioblastoma
- Medulloblastoma
- Oligodendroglioma
327-2. Which of the following is most likely the cell of origin for this neoplasm?
- Astrocyte
- Ependymal cell
- Microglial cell
- Neuron
- Oligodendrocyte
327-3. Which of the following most closely matches the typical length of time from first symptom to death in the average untreated patient?
- 2 months
- 6-12 months
- 3 years
- 5 years
- 10 years
CASE NUMBER 329
[ImageScope] [WebScope]
Clinical History: A 16-year-old girl presented to her pediatrician with a 4-month history of headaches. While she was waiting in the pediatrician’s office, she experienced a seizure. Physical exam revealed coarse vertical nystagmus and papilledema. She died two weeks later.
Image Gallery:
(Summary of Gross Findings - click here)
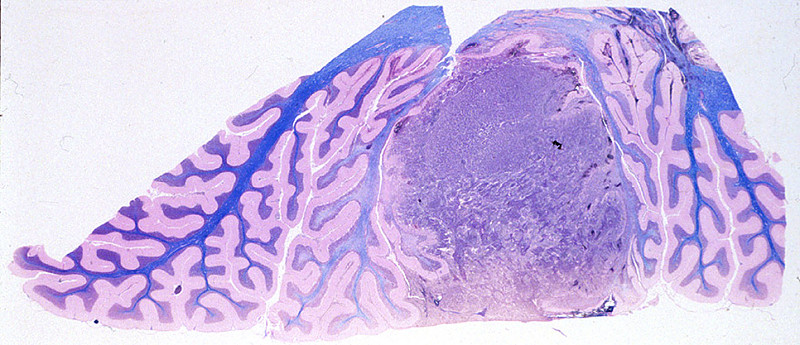
A tumor is present in the cerebellar vermis and compresses the fourth ventricle. It invades the medulla obstructing the flow of CSF.
|
(Summary of Microscopic Findings - click here)
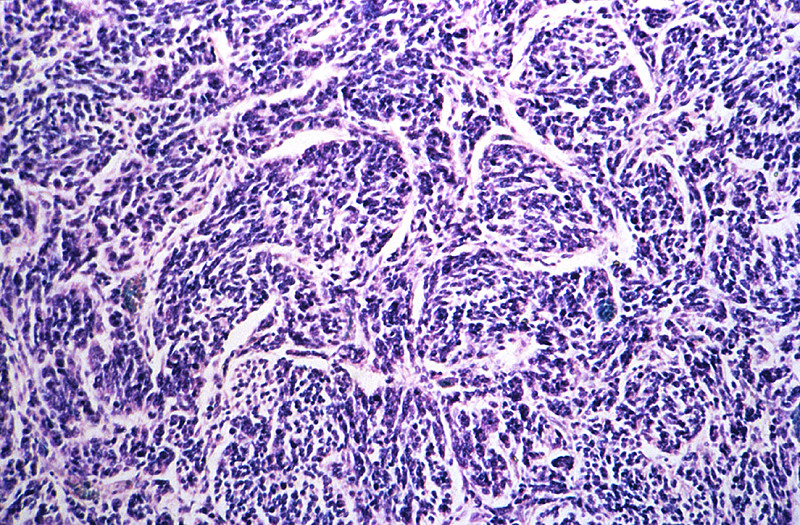
The section shows cerebellum with a pink molecular layer. Underlying that is the Purkinje cell layer composed of large pyramidal neurons. Next is the granular cell layer. Granule cells are neurons. They are the cell on origin of medulloblastoma and are similar in appearance to the tumor cells which are round or oval with dark staining nuclei. Mitotic figures are present. The white matter of the cerebellum stains blue with the H&E/ luxol fast blue stain.
|
(Review Normal Histology - click here)
IV. Cerebellum
Slide 77 20x (cerebellum, H&E) [WebScope] [ImageScope]
Slide 77 40x (H&E) [WebScope] [ImageScope]
Slide 77a 40x (luxol blue/cresyl violet) [WebScope] [ImageScope]
Using slide 77, determine that the cerebellar cortex is organized into an outer molecular layer [example] containing basket and stellate cells (not distinguishable by routine light microscopy) as well as axons of granule cells found in the deeper, highly cellular granule layer [example]. Still deeper is the white matter [example] of the cerebellum, which contains nerve fibers, neuroglial cells, small blood vessels, but no neuronal cell bodies.
Examine the boundary between molecular and granule cell layers. Here you will see the Purkinje cell bodies [example]. In these slides you will not be able to discern the amazing dendritic tree that extends from the Purkinje cell bodies into the molecular layer, nor will you be able to see their axons, which extend down through the granular layer into deeper parts of the cerebellum. The dendritic tree and axon or each Purkinje cell can only be seen in thicker sections stained with special silver stains. Most of the nuclei visible in the granular layer belong to very small neurons, granule cells, which participate in the extensive intercommunication involved in the cerebellum’s role in balance and coordination.
This section of brain is stained with hematoxylin and eosin. The tumor of the left side of the brain was due to the proliferation and infiltration of moderately pleomorphic fibrillary astrocytic cells. There is focal necrosis. Necrosis is the hallmark of glioblastoma. Better differentiated slower growing astrocytomas do not exhibit necrosis. |
329-1. Which of the following is the most likely diagnosis?
- Astrocytoma
- Ependymoblastoma
- Glioblastoma
- Medulloblastoma
- Oligodendroglioma
329-2. Which of the following is the most common site for this tumor to arise?
- Brainstem
- Dura
- Lateral ventricles
- Midline of the cerebellum
- White matter of the cerebral hemispheres
329-3. Which of the following is true regarding this tumor?
- It is extremely resistant to radiation
- It frequently disseminated through the CSF
- It typically follows an indolent clinical course
- MYC amplification is associated with a better prognosis
- The tumor cells are markedly pleomorphic
MUSCLE PATHOLOGY Review Items
Key Vocabulary Terms (click here to search any additional terms on Stedman's Online Medical Dictionary)
LEARNING OBJECTIVES
- Absolutely critical information you must know to practice medicine is in bold font.
- Important information that will be needed for routine patient care is in regular font.
- Information about less common diseases that you may encounter in clinical practice and that will probably appear on examinations is in italics
- Describe the structural features of normal skeletal muscle in terms of:
- gross morphology
- light microscopic appearance
- electron microscopic appearance
- histochemistry
- Describe proper skeletal muscle biopsy procedure, in terms of:
- choice of site
- biopsy technique
- techniques of fixation, processing, staining
- common artifacts seen
- limitations
- Describe the neuromuscular apparatus, and list disease processes and histopatholgic findings of diseases affecting the following components:
- Discuss the clinical approach and appropriate use of diagnostic tests in the evaluation of a patient with a myopathy.
- Describe the ways in which the following factors influence chemical injuries:
- Compare and contrast the clinical and pathologic features of skeletal muscle disorders:
- Compare and contrast the clinical and pathologic features of the following types of muscular dystrophy:
- Duchenne
- Becker
- Myotonic
- limb girdle
- Discuss the clinical and pathologic features of the following disorders:
- spinal muscular atrophy
- glycogenoses
- myasthenia gravis
- Lambert-Eaton myasthenic syndrome
- AIDS-associated myopathy
- viral myositis
- trichinosis
- cysticercosis
- polymyositis
NERVOUS SYSTEM PATHOLOGY Review Items
Key Vocabulary Terms (click here to search any additional terms on Stedman's Online Medical Dictionary)
LEARNING OBJECTIVES
- Absolutely critical information you must know to practice medicine is in bold font.
- Important information that will be needed for routine patient care is in regular font.
- Information about less common diseases that you may encounter in clinical practice and that will probably appear on examinations is in italics
- Describe the morphology and function of the following CNS cells:
|
|
|
- choroid plexus epithelial cells
|
|
|
|
|
- Compare CNS myelin with PNS myelin, in terms of:
- cells of elaboration
- structure and function
- reactions to injury and destruction
- regenerative potential
- Discuss normal CSF in terms of:
- sites of formation
- circulation patterns
- sites of absorption
- pressure
- glucose and protein levels
- cell types present
- Describe the blood-brain barrier (BBB) in terms of:
- physiologic definition
- anatomic counterparts
- morphologic alterations
- areas of absence
- Describe the morphology and function of the following CNS cells:
|
|
|
|
|
|
- ischemic neuronal necrosis
|
|
|
|
|
|
- Compare and contrast the following types of cerebral edema and their significance:
- cytotoxic
- vasogenic
- interstitial
- Compare and contrast the clinical findings and sequelae of herniation of the brain:
- subfalcine (cingulate gyrus)
- transtentorial (uncal)
- foraminal (tonsillar)
- Correlate destructive lesions in specific areas of the CNS with corresponding functional consequences.
- Compare and contrast:
- communicating hydrocephalus
- non-communicating hydrocephalus
- hydrocephalus ex vacuo
- Describe the following congenital abnormalities and their clinical phenotype:
|
- spina bifida/meningomyelocele
|
- Chiari type I malformation
|
|
- Chiari type II (Arnold-Chiari) malformation
|
|
- Dandy-Walker malformation
|
|
|
- agenesis of corpus callosum
|
|
|
|
|
- Compare and contrast genetics, clinical presentation and pathology of inborn errors of metabolism:
|
- spina bifida/meningomyelocele
|
- Chiari type I malformation
|
|
- Chiari type II (Arnold-Chiari) malformation
|
|
- Dandy-Walker malformation
|
|
|
- agenesis of corpus callosum
|
|
|
|
|
- Describe the effects of hypoxia/ischemia on the late gestational/perinatal brain, including the pathophysiologic mechanisms underlying the following:
|
|
- germinal matrix hemorrhage
|
|
- periventricular leukomalacia
|
|
- Discuss the clinical and pathologic features of the following processes:
- Compare and contrast the clinical and pathologic features of CNS aneurysms:
- saccular ("berry"
- atherosclerotic
- Charcot-Bouchard
- mycotic
- Compare and contrast the clinical and pathologic features of CNS vascular malformations:
- arteriovenous malformation
- cavernous angioma
- capillary telangiectasia
- List the ways in which hypertension may harm the brain.
- Compare and contrast the clinical and pathologic features of:
- hypertensive encephalopathy
- hypoxic encephalopathy
- multi infarct dementia
- Compare and contrast the clinical and pathologic features of CNS infarcts:
- nonhemorrhagic (pale, anemic)
- hemorrhagic (red)
- border zone (watershed)
- incomplete
- spinal cord
- Compare and contrast clinical presentations of infarcts in these vascular territories:
- middle cerebral
- vertebrobasilar
- internal carotid
- Describe the interrelationship between hypotension and watershed infarcts.
- Explain the basis of the reperfusion theory of causation of hemorrhagic cerebral infarcts.
- Compare and contrast the clinical and pathologic features:
- skull fracture
- parencymal brain injury
- vascular brain injury
- Compare and contrast open vs. closed head injury, complications and prognosis.
- Compare and contrast the clinical and pathologic features of the following entities:
- pyogenic meningitis
- tuberculous/mycobacterial meningoencephalitis
- viral meningoencephalitis
- fungal meningitis
- neurosyphilis
- neuroborreliosis (Lyme disease)
- rickettsial infection
- protozoal infection
- List the common bacterial agents of acute pyogenic meningitis, and the age group that each most frequently affects.
- Compare and contrast the clinical and pathologic features:
- brain abscess
- subdural empyema
- extradural abscess
- Compare and contrast the clinical and pathologic features of viral meningoencephalitis:
- arboviral encephalitides
- herpes simplex viral encephalitis
- varicella-zoster viral encephalitis
- cytomegalovirus (CMV) encephalitis
- poliomyelitis
- rabies
- human immunodeficiency virus (HIV) infections
- HIV meningoencephalitis (subacute encephalitis)
- vacuolar myelopathy
- progressive multifocal leukoencephalopathy (PML)
- subacute sclerosing panencephalitis (SSPE)
- Discuss the clinical and pathologic features of the following prion diseases:
- Creutzfeldt-Jakob disease (CJD)
- variant CJD (vCJD, "mad cow" disease)
- kuru
- scrapie
- Compare and contrast the clinical and pathologic features degenerative diseases:
|
- olivopontocerebellar atrophy
|
|
|
|
- spinocerebellar degeneration
|
- progressive supranuclear palsy
|
- amyotrophic lateral sclerosis (ALS)
|
- corticobasal degeneration
|
|
- striatonigral degeneration
|
|
|
|
- Describe multiple sclerosis (MS) in terms of:
- geographic distribution
- etiology
- age at onset
- distribution of lesions
- morphology
- clinical course
- Discuss the following nervous system disorders:
|
- carbon monoxide poisoning
|
- acute ethanol intoxication
|
|
|
- central pontine myelinolysis (CPM)
|
|
|
- Discuss the clinical and pathologic features of the following nutritional disorders:
- Wernicke encephalopathy
- Korsakoff psychosis
- neuropathic beriberi
- subacute combined degeneration
- Explain the concepts of benign vs. malignant neoplasms of the CNS.
- Compare and contrast the clinical, pathologic, epidemiologic and genetic features of the following CNS neoplasms:
- colloid cyst of third ventricle
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
- malignant peripheral nerve sheath tumor
|
|
|
- Compare and contrast the clinical, pathologic and genetic features of the following phakomatoses:
|
|
|
|
|
- von Hippel-Lindau syndrome
|
- Discuss the clinical and pathologic features of the following disorders of the PNS:
|
|
|
|
|
- paraproteinemia-associated neuropathy
|
|
|
- AIDS-associated peripheral neuropathy
|
|
- hereditary motor & sensory neuropathy (HMSN)
|
|
- type I [Charcot-Marie-Tooth disease (CMT) 1]
|
|
- type III (Dejerine-Sottas disease)
|
|
EYE PATHOLOGY Review Items
Key Vocabulary Terms (click here to search any additional terms on Stedman's Online Medical Dictionary)
LEARNING OBJECTIVES
- Absolutely critical information you must know to practice medicine is in bold font.
- Important information that will be needed for routine patient care is in regular font.
- Information about less common diseases that you may encounter in clinical practice and that will probably appear on examinations is in italics
- Discuss the anatomy of the orbit and name the important compartments and tissues.
- Describe ocular findings in the following congenital conditions:
- trisomy 13
- trisomy 21
- congenital rubella
- congenital syphilis
- Discuss the clinical and pathologic features of inflammatory conditions of the eye and orbit:
|
|
|
|
|
|
|
|
|
- granulomatous inflammation
|
|
- sympathetic ophthalmia (uveitis)
|
- Compare and contrast the clinical and pathologic features of glaucoma:
- congenital
- primary angle-closure
- secondary angle closure
- open-angle
- Discuss the clinical and pathologic features of the following degenerative conditions:
- Discuss cataracts with regard to:
- associated diseases
- etiology
- classification
- morphology
- Discuss the clinical and pathologic features of the following diseases:
- retinopathy of prematurity (retrolental fibroplasia)
- retinitis pigmentosa
- macular degeneration
- retinal detachment
- Compare and contrast the clinical and pathologic features of he following vascular disorders:
- central retinal artery occlusion
- central retinal vein occlusion
- hypertensive retinopathy
- arteriosclerotic retinopathy
- diabetic retinopathy
- Describe the ocular lesions associated with:
- vitamin A deficiency
- methanol toxicity
- List the most frequent primary and metastatic malignancies of the:
- eyelid
- conjunctiva
- uvea (uveal tract)
- optic nerve
- Discuss the clinical and pathologic features of the following malignancies of the eye:
- malignant melanoma
- retinoblastoma
- metastatic malignancy
- Discuss the clinical and pathologic features of diseases of the optic nerve:
- papilledema
- optic neuritis
- optic atrophy
- Name the two most common causes of blindness in the world and the four most common causes of blindness in the United States
|