CASE NUMBER 18
[ImageScope] [WebScope]
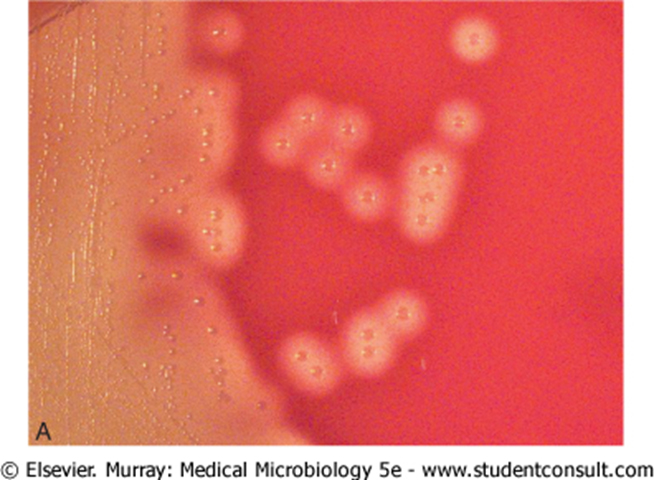
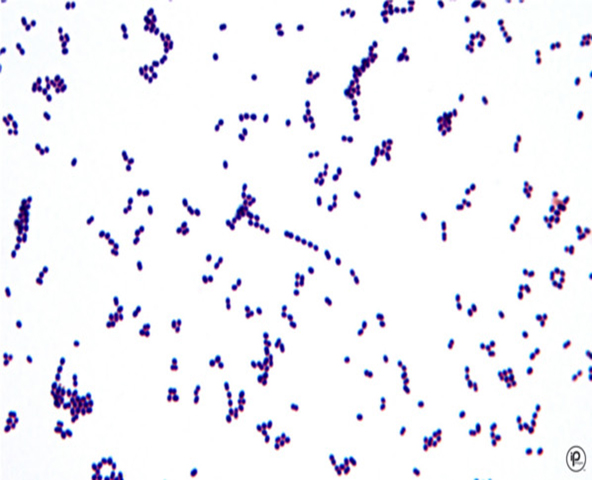
Clinical History: A 29-year-old man presented to his primary care physician with a sore throat and “flu-like” symptoms. A gross image of his oral cavity is shown as are culture specimens and a Gram stain of organisms scraped from his tonsils.
Image Gallery:
18-1. What is the differential diagnosis?
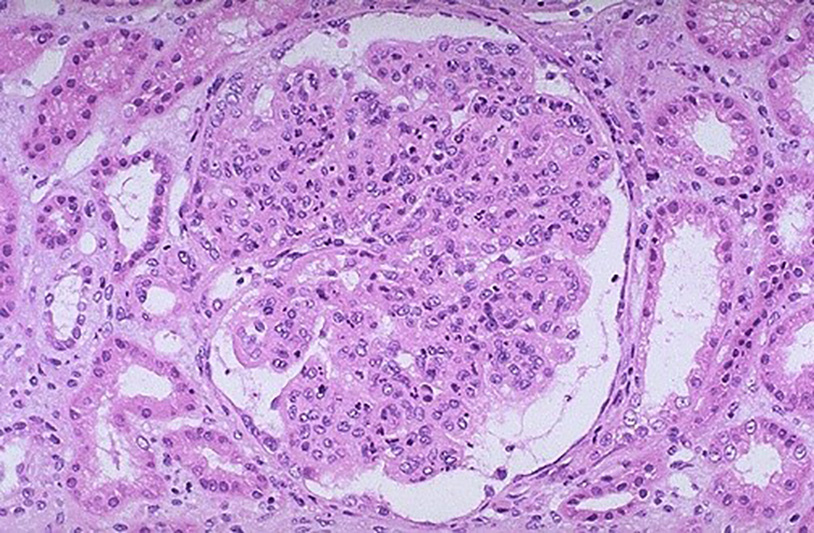
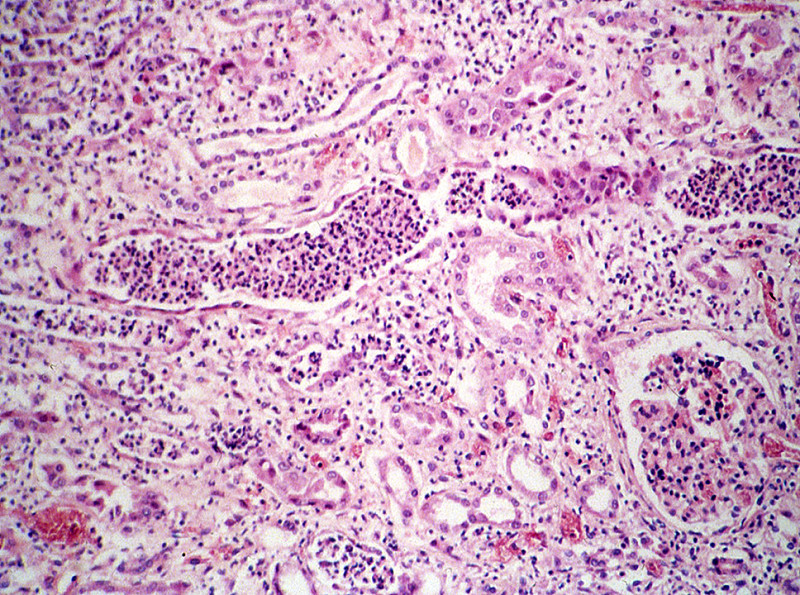
Clinical History (continued): Two weeks later, the patient returned to his primary care physician and reported that his urine appeared dark and that he had been urinating less frequently than usual. Physical exam showed periorbital edema and blood pressure of 200/120 mm Hg. Urinalysis revealed hematuria with red blood cell casts, and moderate proteinuria. His BUN was 180 mg/dL (normal 7-21 mg/dL). A biopsy of his kidney is shown below.
18-2. What is the differential diagnosis?
18-3. Which of the following is the appropriate term for the clinical complex of 1) hematuria; 2) oliguria and azotemia; and 3) hypertension?
- Hemolytic uremic syndrome
- Malignant hypertension
- Nephritic syndrome
- Nephrotic syndrome
- Thrombotic thrombocytopenic purpura
18-4. Which of the following is a characteristic finding in patients with this disease?
- Diffuse thickening of the capillary wall
- Linear deposits of IgG
- Mesangial deposition of IgA
- Subepithelial “humps” seen on electron microscopy
- “Tram track” appearance of the glomerular basement membrane
CASE NUMBER 9
[ImageScope] [WebScope]
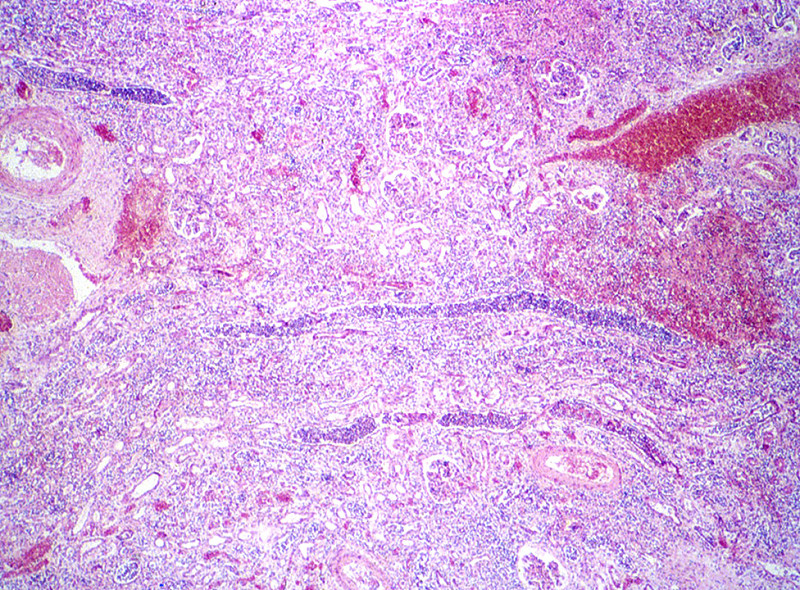
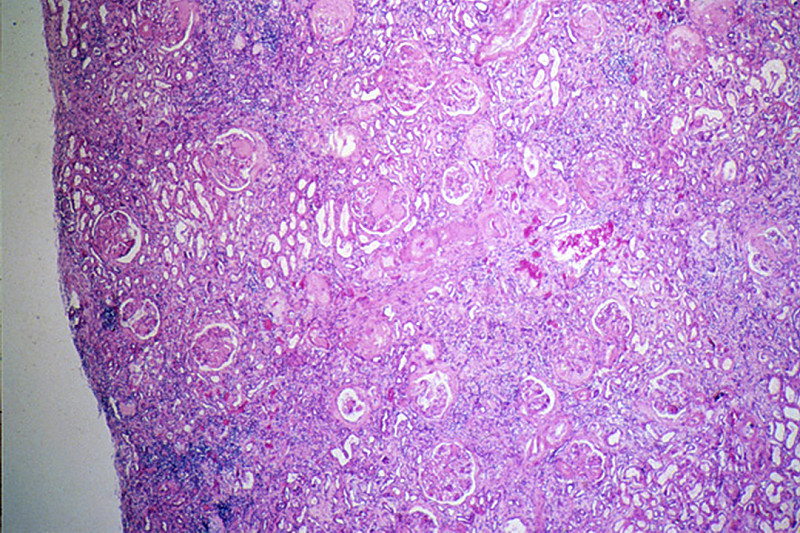
Clinical History: A 51-year-old diabetic man presented to his primary care physician with a 3-week history of urinary frequency and incontinence. He reported that he had had multiple urinary tract infections over the previous year that had been treated with antibiotics. Urinalysis was positive for WBCs and bacteria. Physical exam revealed mild bilateral lower extremity weakness. A screening CT scan showed a small spinal cord tumor at T11 and the patient underwent surgery; however, postoperatively he developed fever and costovertebral angle tenderness that did not respond to antibiotics. He died on post-operative day 3. A catheterized urine specimen was obtained before death. Culture showed colonies on blood agar and on MacConkey agar. Gram stain of a blood culture showed gram-negative rods.
Image Gallery:
|
|
(Review Normal Histology - click here)
Norm No. 2 Kidney
[ImageScope] [WebScope]
The kidney excretes soluble waste from the body and controls electrolyte balance. It consists of the cortex and the medulla. Within the outer cortex, glomeruli with delicate capillary loops are seen. The basement membrane is thin and without inflammation or thickening. Bowman’s capsule that surrounds the glomerulus is thin. The interstitium demonstrates no evidence of inflammation or fibrosis. In the areas between the glomeruli, tubules and arterioles are seen. The tubules are intact. The vessels exhibit no narrowing or wall thickening. The inner medulla of the kidney contains only tubules and blood vessels. Larger arteries and veins are located at the interface between cortex and medulla.
|
9-1. What is the differential diagnosis?
9-2. Which of the following is the most common causative organism in this disease?
- Adenovirus
- Escherichia coli
- Mycobacterium tuberculosis
- Staphylococcus aureus
- Streptococcus pneumoniae
9-3. Which of the following is the most common etiology of this disease in young children?
- Arterionephrosclerosis
- Autoantibodies to ADAMTS 13
- Gout
- Shiga toxin
- Vesicoureteral reflux
9-4. In the context of this disease, papillary necrosis is most closely linked with which of the following?
- Alcohol abuse
- Diabetes
- Male sex
- Neurogenic bladder
- Smoking
CASE NUMBER 20
[ImageScope] [WebScope]
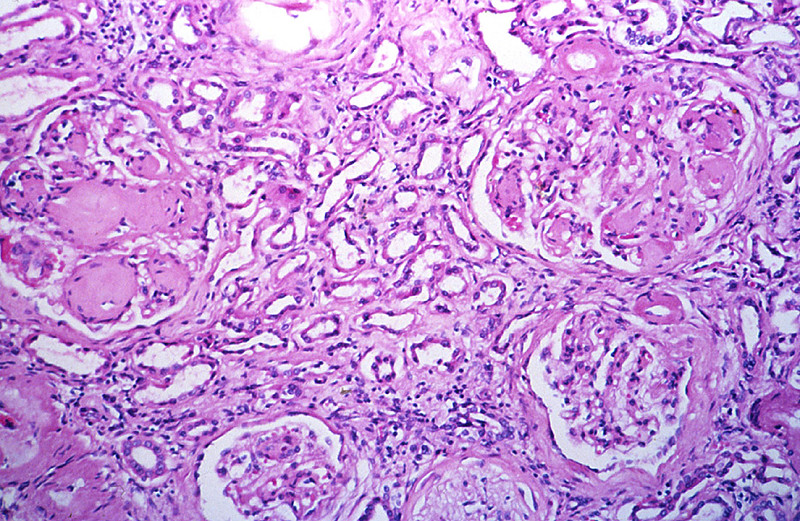
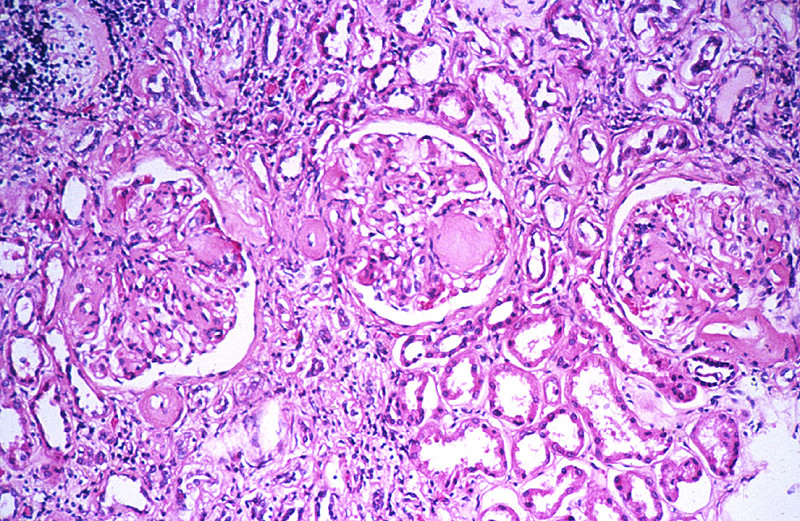
Clinical History: A 15-year old girl presented to her pediatrician with a two-week history of frequent urination, increased thirst and weight loss. Following evaluation, she was diagnosed with insulin-dependent diabetes and was placed on insulin therapy. She was non-compliant with her medication, however, and was found in a coma one morning. Laboratory values at hospital admission were blood sugar of 300 mg/dL, serum bicarbonate of 9 mEq/L, and blood pH of 6.9. Despite aggressive therapy, the patient died.
Image Gallery:
|
|
(Review Normal Histology - click here)
Norm No. 2 Kidney
[ImageScope] [WebScope]
The kidney excretes soluble waste from the body and controls electrolyte balance. It consists of the cortex and the medulla. Within the outer cortex, glomeruli with delicate capillary loops are seen. The basement membrane is thin and without inflammation or thickening. Bowman’s capsule that surrounds the glomerulus is thin. The interstitium demonstrates no evidence of inflammation or fibrosis. In the areas between the glomeruli, tubules and arterioles are seen. The tubules are intact. The vessels exhibit no narrowing or wall thickening. The inner medulla of the kidney contains only tubules and blood vessels. Larger arteries and veins are located at the interface between cortex and medulla.
|
20-1. What is the differential diagnosis?
20-2. Which of the following is the most prominent glomerular lesion in this patient?
- Crescentic proliferation of parietal epithelial cells
- Lipid droplets
- Mesangial IgA deposits
- Nodular glomerulosclerosis
- Subendothelial deposits
20-3. Basement membrane thickening in the eye and kidney is believed to occur through which one of the following processes?
- Activation of protein kinase C
- Disturbance in the polyol pathway
- Excess glutathione due to increased NADPH
- Increased production of vascular endothelial growth factor
- Protein crosslinking mediated by advanced glycation end productions
20-4. Which of the following is the most common cause of end stage renal disease?
- Analgesic nephropathy
- Diabetes mellitus
- Hypertension
- Polycystic kidney disease
- Systemic lupus erythematosus
CASE NUMBER 2
[ImageScope] [WebScope]
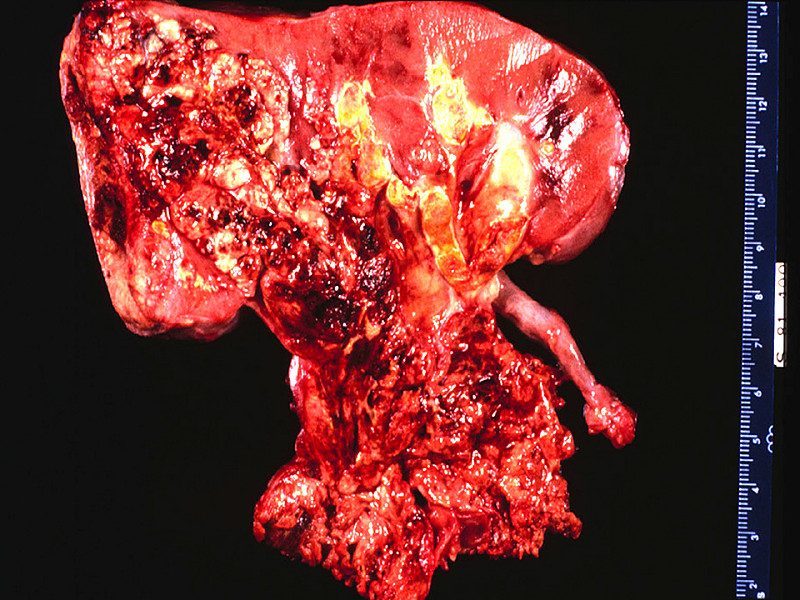
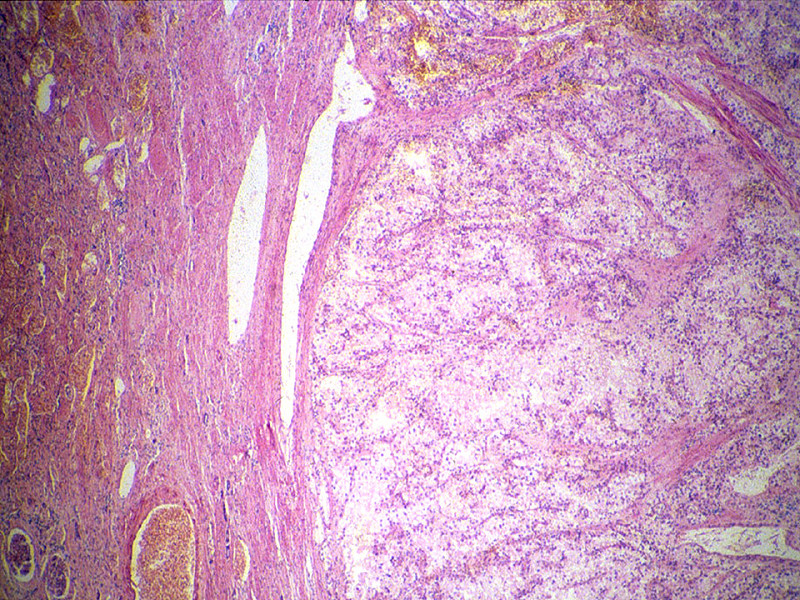
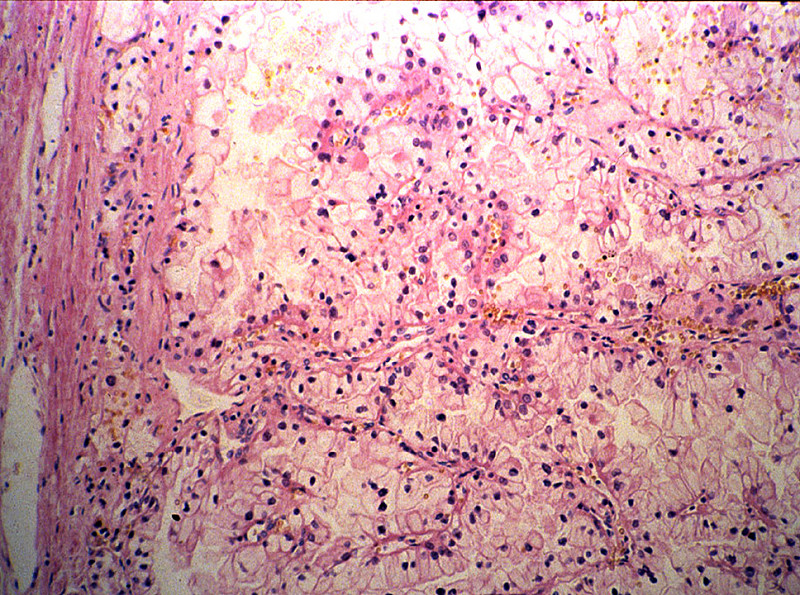
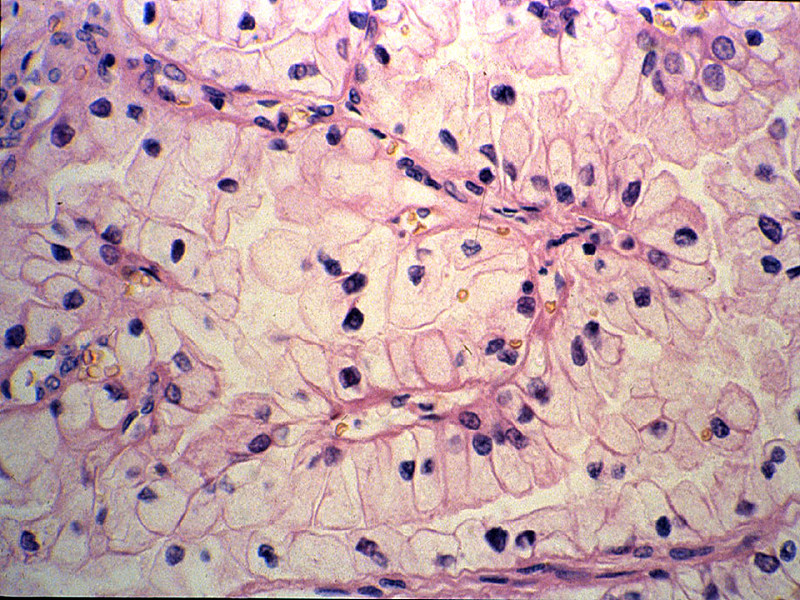
Clinical History: This 45-year-man noticed blood in his urine. His physician ordered a CT of the lower abdomen and pelvis. A mass in the superior pole of the kidney was discovered. A biopsy was performed and then the kidney was removed.
Image Gallery:
|
|
(Review Normal Histology - click here)
Norm No. 2 Kidney
[ImageScope] [WebScope]
The kidney excretes soluble waste from the body and controls electrolyte balance. It consists of the cortex and the medulla. Within the outer cortex, glomeruli with delicate capillary loops are seen. The basement membrane is thin and without inflammation or thickening. Bowman’s capsule that surrounds the glomerulus is thin. The interstitium demonstrates no evidence of inflammation or fibrosis. In the areas between the glomeruli, tubules and arterioles are seen. The tubules are intact. The vessels exhibit no narrowing or wall thickening. The inner medulla of the kidney contains only tubules and blood vessels. Larger arteries and veins are located at the interface between cortex and medulla.
|
2-1. What is the differential diagnosis?
2-2. Which of the following risk factors is most closely linked to the development of this disease?
- African-American ethnicity
- Alcoholism
- Diabetes mellitus
- Mutations in the PKHD1 gene
- Tobacco abuse
2-3. A 35-year-old woman presented to her primary care physician with a two-week history of headaches and dizziness. An MRI of the brain revealed a cystic posterior fossa mass with a mural nodule; biopsy confirmed a diagnosis of hemangioblastoma. Additional imaging studies revealed a 3 cm mass in the superior pole of the left kidney and a 2.5 cm mass in the inferior pole of the right kidney. A biopsy of the right kidney mass was diagnosed as clear cell renal carcinoma. Which of the following genes is most likely mutated in this patient?
- COL4A3
- MET
- PKD1
- TSC1
- VHL
CASE NUMBER 607
(no virtual slides for this case)
Clinical History: A 45-year old man comes to the emergency department in obvious severe pain. He states that he has severe pain in his left flank that extends down to his left groin. The pain is sharp and severe, and it started several minutes earlier.
607-1. What is the differential diagnosis?
607-2. What tests would you order?
- Abdominal X-ray
- Chest X-ray
- EKG
- Intravenous pyelogram
- MRI of the flank
Clinical History (continued): An abdominal radiograph is obtained as shown below.
Image Gallery:
607-3. What is the differential diagnosis?
607-4. Which of the following is the most likely composition of the radiographic feature indicated by the arrow on the radiograph?
- Ammonium magnesium phosphate
- Calcium
- Cystine
- Uric acid
CASE NUMBER 13
(no virtual slides for this case)
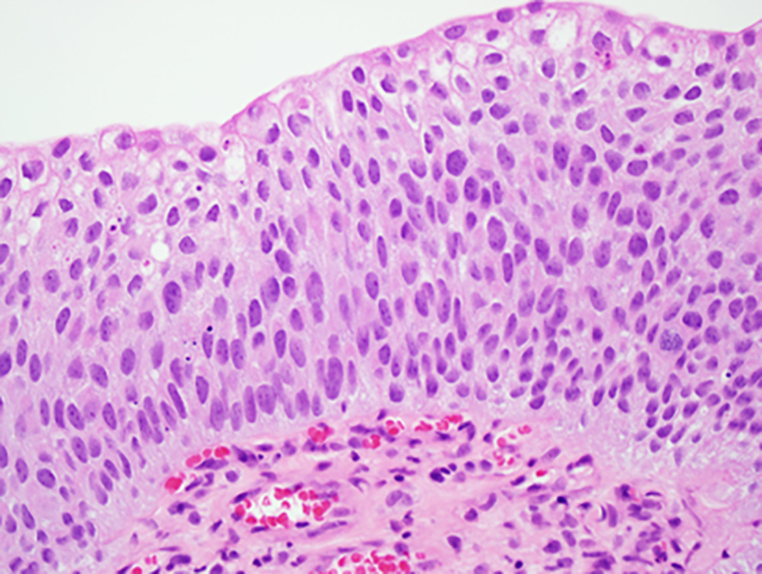
Clinical History: A 57-year-old man presented to his primary care physician after an episode of painless hematuria. Cystoscopy was performed and a mass was noted near the dome of the bladder.
Image Gallery:
13-1. What is the differential diagnosis?
13-2. Which of the following is the most significant risk factor in the development of this lesion?
- Arylamine exposure
- Bladder stones
- Cigarette smoking
- Schistosomiasis
- VHL mutation
13-3. A 35-year-old woman from Angola presents to her primary care physician following an episode of painless hematuria. A routine blood test revealed eosinophilia and subsequent ELISA analysis confirmed a diagnosis of schistosomiasis. This patient is at greatest risk for developing which of the following?
- Adenocarcinoma
- Papilloma
- Papillary urothelial carcinoma
- Small cell carcinoma
- Squamous cell carcinoma
RENAL PATHOLOGY Review Items
Key Vocabulary Terms (click here to search any additional terms on Stedman's Online Medical Dictionary)
LEARNING OBJECTIVES
Absolutely critical information you must know to practice medicine is in bold font.
Important information that will be needed for routine patient care is in regular font.
Information about less common diseases that you may encounter in clinical practice and that will probably appear on examinations is in italics
- List the clinical criteria for diagnosis and pathology
- Discuss the proper use of the following laboratory tests in the evaluation of urinary tract disease and interpret abnormalities of these parameters in clinical context:
- creatinine
- urea (blood urea nitrogen, BUN)
- urinalysis
- Discuss the clinical and pathologic features of the following congenital renal anomalies:
- Compare and contrast the clinical and pathologic features of cystic diseases of the kidney:
- Define the following terms as they apply to glomerular histopathology:
- Discuss clinical and pathologic features of the following glomerular diseases:
- Describe the major clinical and histopathologic findings associated with renal involvement by the following systemic diseases:
- Discuss lupus nephritis in terms of:
- etiology and pathogenesis
- clinical presentation
- nomenclature, morphologic features, and prognosis of each of the five classes
- Discuss the clinical and pathologic features of renal tubular diseases:
- Discuss the significance of unilateral renal artery disease, including:
- usual causes
- mechanism(s) of clinical effects
- morphologic changes in contralateral kidney
- tests used for detection and localization
- Describe the pathophysiology of hypertension induced by renal artery constriction
- Compare and contrast benign and malignant nephrosclerosis with regard to:
- pathogenesis
- morphologic (gross and microscopic) appearance
- clinical presentation, course, and prognosis
- List the three major thrombotic microangiopathies; describe the renal effects and pathogenesis in terms of:
- microscopic appearance
- clinical presentation, course, and prognosis
- Discuss renal vein thrombosis in terms of:
- etiology/pathogenesis
- morphology
- method(s) of diagnosis
- clinical and laboratory features
- Discuss urolithiasis in terms of:
- composition and relative incidence of various types of stones
- pathophysiologic abnormalities associated with the common types of stones
- etiology and pathogenesis of stone formation
- effect of location of stones on clinical and anatomic findings
- clinical course and complications
- Discuss hydronephrosis in terms of:
- etiologic factors and their relative frequencies
- pathogenesis
- morphology (gross and microscopic)
- clinical course and prognosis
- Discuss the following renal neoplasms:
LOWER URINARY TRACT PATHOLOGY Review Items
Key Vocabulary Terms (click here to search any additional terms on Stedman's Online Medical Dictionary)
LEARNING OBJECTIVES
Absolutely critical information you must know to practice medicine is in bold font.
Important information that will be needed for routine patient care is in regular font.
Information about less common diseases that you may encounter in clinical practice and that will probably appear on examinations is in italics
- Describe the normal anatomy (gross and microscopic) of each of the following:
- Discuss the proper use of urinalysis in the evaluation of lower urinary tract disease, and interpret abnormalities of this test in clinical context
- Discuss obstruction at various levels of the urinary tract in terms of:
- site and nature of lesion
- etiology and pathogenesis
- alteration in renal function
- morphologic effect on kidney
- Discuss diverticula of the urinary bladder, in terms of:
- etiology
- pathogenesis
- morphology
- complications
- Discuss urolithiasis in terms of:
- relative incidence of various types of stones
- pathophysiologic abnormalities associated with the common types of stones
- etiology and pathogenesis of stone formation
- effect of location of stones on clinical and anatomic findings
- clinical course and complications
- Discuss the clinical and pathologic features of the following congenital anomalies:
- patent urachus
- hypospadias
- eductivepispadias
- exstrophy of the bladder
- duplications of the collecting system
- urethral valves
- Compare and contrast clinical and pathologic features of inflammatory conditions:
- infectious cystitis
- interstitial cystitis
- malacoplakia
- Compare and contrast the clinical and pathologic features of lower urinary tract neoplasms
- urothelial (transitional cell) carcinoma
- squamous cell carcinoma
- adenocarcinoma
|