|
|
Pathology of Infectious Diseases Slide list:
Slide Descriptions Slide 4-01. Adenovirus infection, liver Adenovirus replication occurred unchecked in this patient with severe combined immunodeficiency, leading to destruction of much of the liver. Hepatocytes with bizarre smudgy nuclei that are adjacent to the necrotic regions are adenovirus-infected cells.
Slide 4-02. Fungal abscess, lung The lesion extends through the pleural surface of the lung. Note the ring of neutrophils that surround the mass of necrotic tissue. The fungal hyphae can be seen quite well, particularly at the edges of the abscess, despite the lack of specific fungal staining.
Slide 4-03A. Fungal thrombosis and abscess, lung, silver Slide 4-03B. Fungal thrombosis and abscess, lung, H&E Note the fungus-filled vessels in the center of the one of the 2 abscesses present. The accompanying methenamine silver stain highlights the fungal hyphae, but they can be seen quite well on the H & E-stained section. The section of bronchus demonstrates extensive squamous metaplasia. The remaining normal respiratory epithelial cells have enlarged nuclei, some with nuclear inclusions, consistent with viral infection. Parainfluenza virus was cultured from this patient and bronchial infection was confirmed by immunostaining.
Slide 4-04A. Parainfluenza virus infection, lung, H&E
Slide 4-04B. Parainfluenza virus infection, lung, silver The section demonstrates areas of hemorrhage and organizing pneumonia with numerous giant cells resulting from parainfluenza virus infection. The giant cells are formed by fusion of virally-infected alveolar epithelial cells. Note on the accompanying immunostain that all giant cells do not react with the parainfluenza virus antibody. It is not known if this is artefactual or if it reflects the particular stage in the life cycle of the virus within those cells. Also note that a brown color does not always represent positive immunostaining, since hemosiderin-laden macrophages are also common in this section.
Additional slides from the Duke Medical School Pathology Teaching Collection: CASE NUMBER 39 Clinical History: A 58-year-old female had been hemiplegic on the right for a period of 3 months prior to death. She developed fever and dyspnea several days prior to death. Gross: There was a thrombosis of the left internal carotid artery with infarction of the left cerebral hemisphere. There was a massive embolus of the right pulmonary artery. Both lungs were firm with mucopurulent exudate in and about the bronchi. The left lower lobe was firm and gray-yellow with a shaggy fibrinous exudate over the pleura. (E. Coli and Proteus mirabilis were cultured from this area). Microscopic: Bronchi and alveoli are filled with neutrophils. There are scattered masses of fibrin. DIAGNOSIS: Bronchopneumonia
Image Gallery:
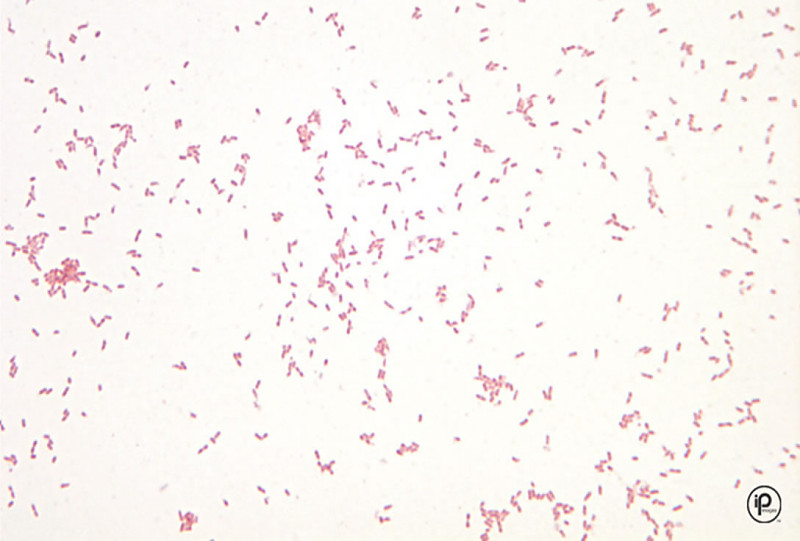
CASE NUMBER 281 Clinical History: A 47-year-old female had an eight-year history of refractory anemia and pancytopenia. She was treated with steroids. She was admitted shortly before death with fever and signs of infection. Gross: Multiple discrete nodules of the lung parenchyma along with thrombosed vessels were observed. Microscopic: The tissue reaction to the fungus infection cannot be seen well with this methenamine silver stain. It does bring out well the appearance of the Aspergillus with its septate hyphae and radial pattern of growth. DIAGNOSIS: Aspergillosis, Lung
Image Gallery:
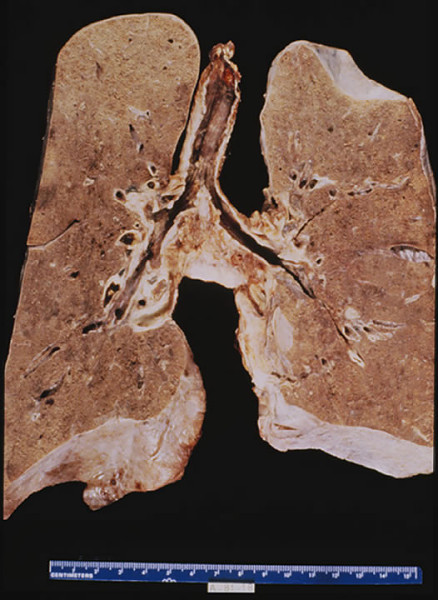
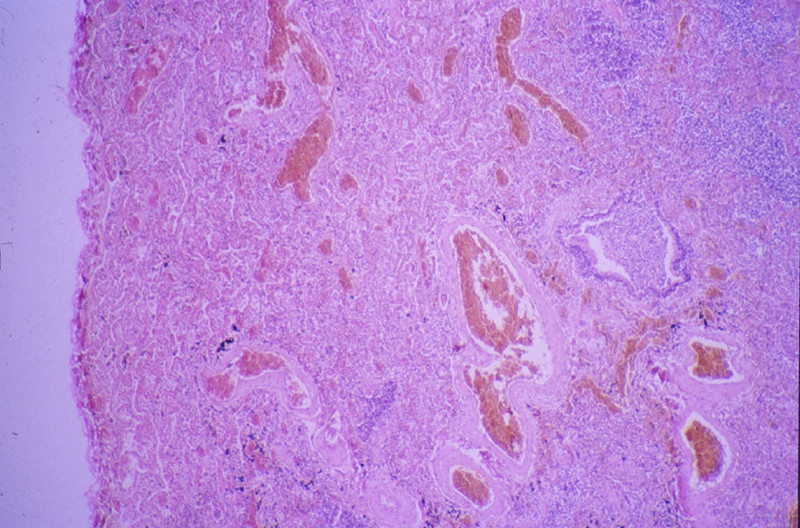
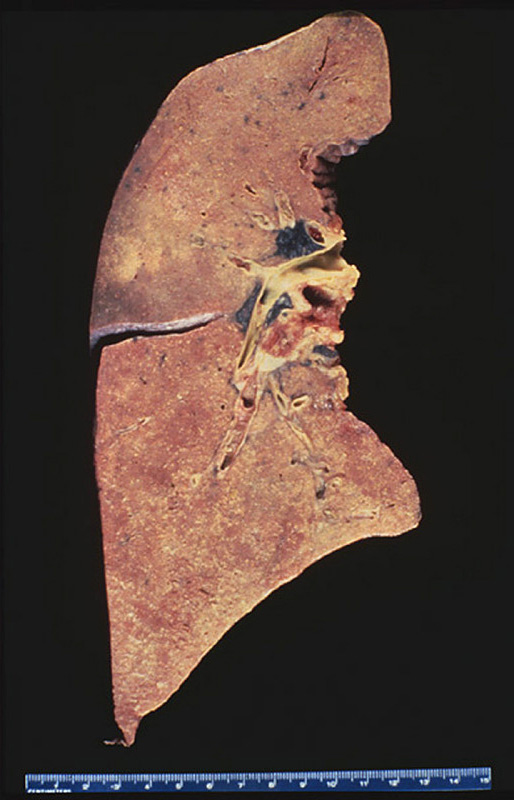
CASE NUMBER 451 Clinical History: A 4-year-old female had a gradual onset of fever, productive cough, anorexia and diarrhea about eleven days prior to death. The breathing sounds were harsh, and a few cracking rales were heard over the right base posteriorly. Gross: The lungs showed fibrinous exudates over the pleural surfaces. The cut surface of the lung revealed innumerable small, gray-white nodules 1-4 mm in size. A large caseous tubercle of 0.5 cm was present in the left lower lobe, eroding into a large pulmonary vessel. Microscopic: A lower power examination reveals numerous poorly defined tubercles approximately of the same size and same stage of development. These tubercles show a slight caseous necrosis and consist predominantly of mononuclear cells, epitheloid cells, and a few giant cells. In alveoli there is a moderate amount of mononuclear cell infiltration. Some lymphocyte and plasma cell infiltration is diffusely present in the alveolar septa. DIAGNOSIS: Miliary Tuberculosis of Lung
Image Gallery:
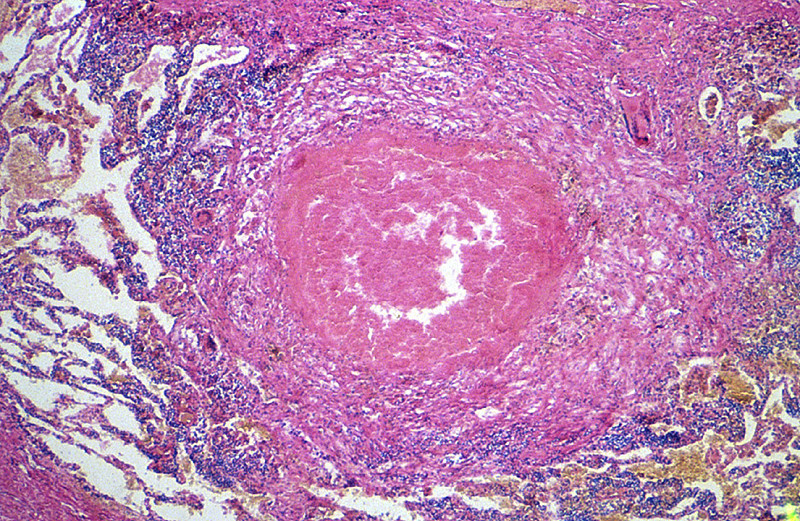
CASE NUMBER 452 Clinical History: A 50-year-old female had chronic cough, chest pain, night sweats and a swollen abdomen for the past four years. Gross: The lungs were heavy and had fibrous pleural adhesions. A large cavity containing caseous material was found in the apex of the left lung. The cavity communicated with a bronchus. In the left lower lobe there was large area of consolidation, which exuded creamy, yellow-gray, caseous material from the cut surface. Microscopic: This section shows many foci of caseous necrosis, which is associated with marked proliferation of histiocytes around the caseous foci. A small bronchus (not present in all sections) shows squamous metaplasia. DIAGNOSIS: Caseous Pulmonary Tuberculosis
Image Gallery:
|
||