|
|
Inflammation and Tissue Repair Slide list:
Slide Descriptions Slide 2-01. Ulcer, stomach The gastric epithelium has been artifactually lost over both of these sections. Nonetheless, it is easy to identify the location of the ulcer, where the mucosa has been lost. The remaining tissue at the ulcer site (called the ulcer bed) is composed of granulation tissue, along with acute and chronic inflammation. Bacterial colonies are evident in tissue adjacent to the ulcer.
Slide 2-02. Bronchopneumonia The 2 sections of lung show patchy consolidation. Affected alveoli are packed with inflammatory cells, including neutrophils. Other alveoli show evidence of edema, with pale pink-staining fluid present within the alveoli.
Slide 2-03. Ulcer, esophagus; Stomach The section of stomach is mostly normal. Normal stratified squamous epithelium is present on one end of each of the 2 sections of esophagus, however the epithelium is absent from the middle and other end of the tissue. The tissue underlying the epithelial defect contains numerous inflammatory cells, many small blood vessels, and plump fibroblasts that are synthesizing collagen. These are characteristics of granulation tissue that characterizes the ulcer bed.
Slide 2-04. Lobar pneumonia Alveoli are uniformly filled with an inflammatory infiltrate consisting of neutrophils, macrophages, lymphocytes, and erythrocytes.
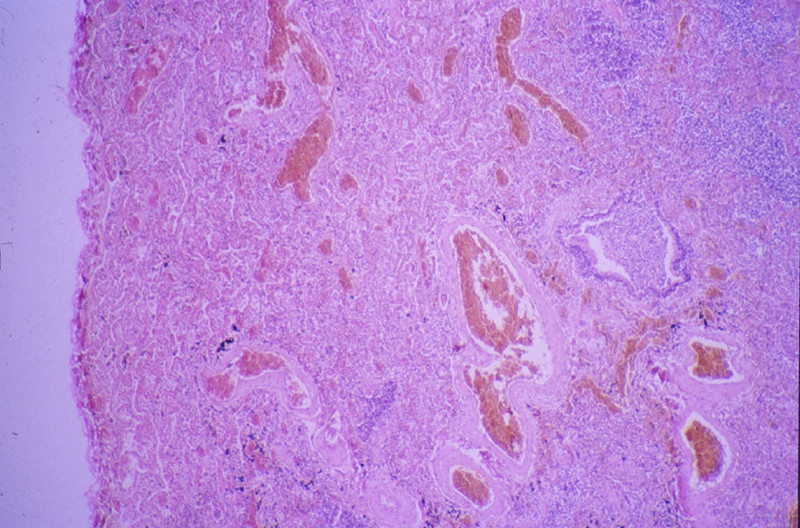
Additional slides from the Duke Medical School Pathology Teaching Collection: CASE NUMBER 17 Gross: The kidneys were small (80 and 90 grams), and were pale and finely granular. The cortex was markedly thinned. Microscopic: All of the 4 main constituents of the kidney (glomeruli, tubules, vessels, and interstitial tissue) are involved. Although all glomeruli are abnormal, they are not involved to the same degree; some are completely replaced by fibrous tissue, others are only partly scarred, and a few still contain patent capillary loops. The latter have increased mesangial and epithelial cells of Bowman's capsule. The tubules are dilated; some contain red blood cells, but most contain hyaline casts. The interstitial tissue is rather diffusely infiltrated with many lymphocytes and plasma cells. There is a moderate to marked degree of arteriolarsclerosis. DIAGNOSIS: Proliferative Glomerulonephritis, Severe, Advanced (Chronic) Image Gallery:
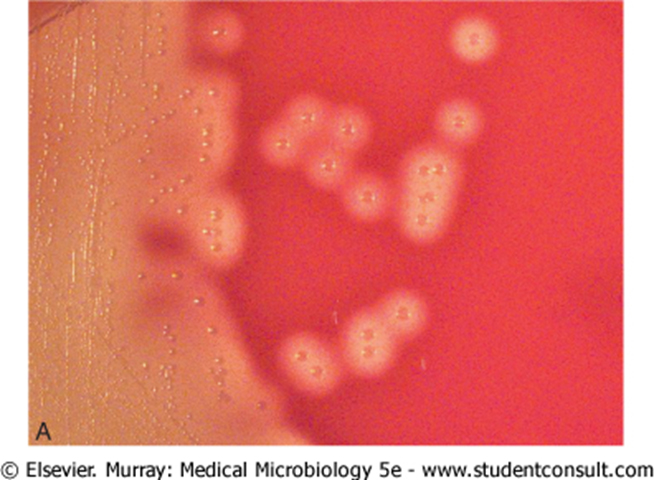
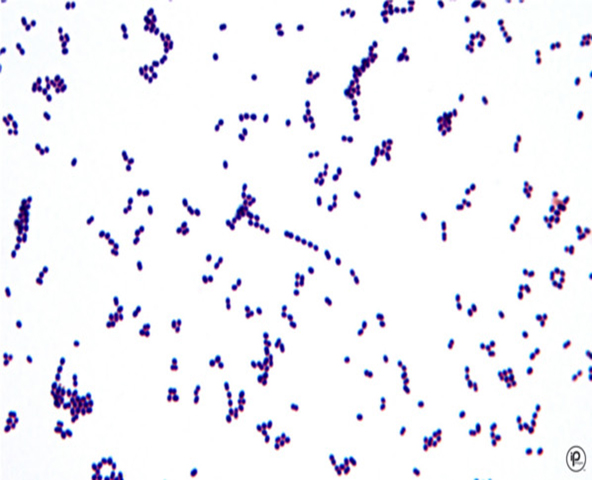
CASE NUMBER 39 Clinical History: A 58-year-old female had been hemiplegic on the right for a period of 3 months prior to death. She developed fever and dyspnea several days prior to death. Gross: There was a thrombosis of the left internal carotid artery with infarction of the left cerebral hemisphere. There was a massive embolus of the right pulmonary artery. Both lungs were firm with mucopurulent exudate in and about the bronchi. The left lower lobe was firm and gray-yellow with a shaggy fibrinous exudate over the pleura. (E. Coli and Proteus mirabilis were cultured from this area). Microscopic: Bronchi and alveoli are filled with neutrophils. There are scattered masses of fibrin. DIAGNOSIS: BronchopneumoniaImage Gallery:
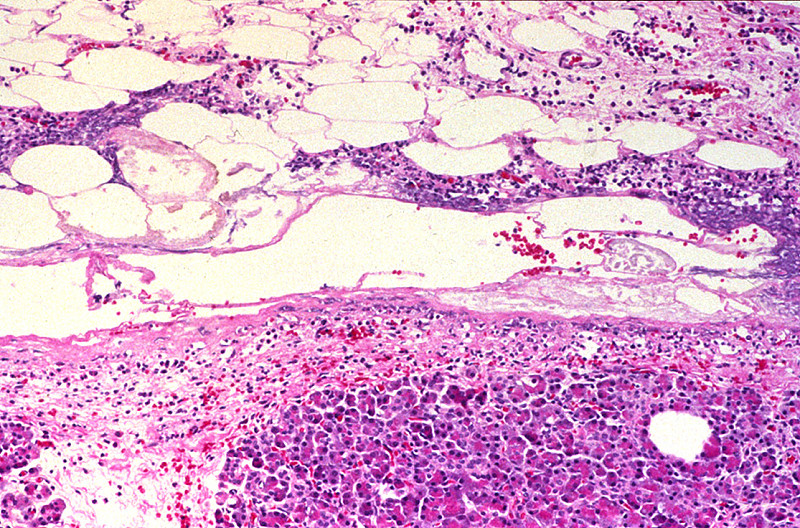
CASE NUMBER 46 Gross: Both lungs were heavy, firm, and dark red. There were numerous firm gray areas up to 0.3 cm. in all lobes. Microscopic: The alveoli were filled with eosinophilic material representing fibrin. There is early proliferation of fibroblasts in some of these areas. At the periphery there are neutrophils and mononuclear cells. Note the marked alveolar hemorrhage. Brown, granular pigment is present in scattered macrophages. This is hemosiderin. Alveolar hemorrhage may be related to the acute glomerulonephritis that was also present in this patient. Note the diffuse neutrophilic infiltrate in alveolar walls. DIAGNOSIS: Organizing Bronchopneumonia Image Gallery:
CASE NUMBER 54 Clinical History: An 18-year-old female had nausea, vomiting, periumbilical and lower abdominal pain, shaking chills and fever beginning two days ago. The WBC count was 21,900. Physical examination revealed local tenderness and rigidity with rebound pain in the lower abdomen. Gross: The appendix was swollen, dark red, hemorrhagic, and covered by gray-yellow exudate. Serial cross-sections revealed a distended lumen containing hemorrhagic material and a fecalith, which apparently obstructed the lumen. Microscopic: Portions of the mucosa are ulcerated, necrotic and heavily infiltrated with neutrophils. This acute inflammation and necrosis extends throughout the entire thickness of the wall and the serosa. In the appendicial lumen there is pus and a fecalith. DIAGNOSIS: Acute Suppurative Appendicitis with Perforation Image Gallery:
CASE NUMBER 81 Clinical History: This 62-year-old male had a history of alcoholism. Two months prior to death he vomited blood. One month before death there was a massive gastrointestinal hemorrhage. He expired following an attempt to ligate esophageal varices. Gross: The liver weighed 1800 grams. The entire organ was uniformly composed of nodules about 0.5 cm in diameter, each surrounded by fibrous tissue. The organ was jaundiced and firm. Microscopic: The usual architecture present in the liver has been completely disrupted by the bands of connective tissue. In these bands one sees chronic inflammatory cells, mainly lymphocytes and other mononuclear cells. There is some proliferation of the bile ductules. DIAGNOSIS: Micronodular Cirrhosis Image Gallery:
CASE NUMBER 89 Clinical History: This 73-year-old female presented with right upper quadrant pain and elevated WBC count. Physical exam revealed right upper quadrant tenderness. Ultrasound examination of the gallbladder revealed gallstones. Gross: The gallbladder was thickened and hyperemic. No localized masses were seen. The gallbladder contained numerous gallstones. Microscopic: The gallbladder mucosa is acutely inflamed with many neutrophils in the epithelium and lamina propria. The epithelium is reactive with enlarged nuclei and abundant eosinophilic cytoplasm and ulcerated in some areas. There is hemorrhage and fibroblastic proliferation throughout the wall. Chronic cholecystitis is evidenced by plasma cells in the mucosa and Rokitansky-Aschoff sinuses which are diverticular invaginations of mucosa in the gallbladder wall. No tumor is seen. DIAGNOSIS: Acute and Chronic Cholecystitis Image Gallery:
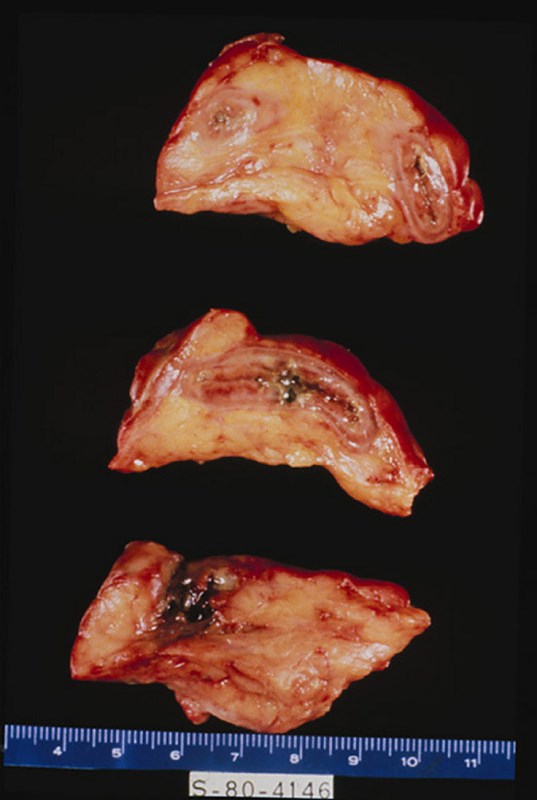
CASE NUMBER 93 Clinical History: A 30-year-old female had recurrent bouts of severe abdominal pain accompanied by elevated serum amylase. Partial pancreatectomy was performed for relief of chronic pain, unresponsive to medical therapy. Gross: Fibrosis obscured some areas of pancreas architecture. Saponification of peripancreatic fat was seen in small foci. Microscopic: Several areas of fat necrosis with adjacent neutrophil infiltrate are seen, evidence of acute pancreatitis. In addition, some lobules of the pancreas show fibrosis and loss acini, evidence of chronic pancreatitis. In these areas, islets of Langerhans appear larger and more abundant. This is partly because they are resistant to injury and persist when acini are destroyed and partly because they undergo reactive hyperplasia DIAGNOSIS: Acute and Chronic Pancreatitis Image Gallery:
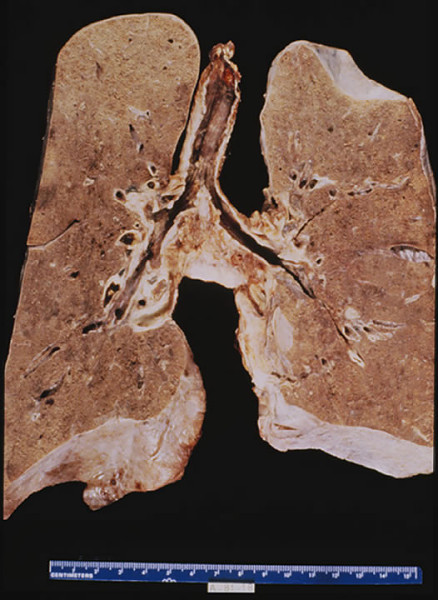
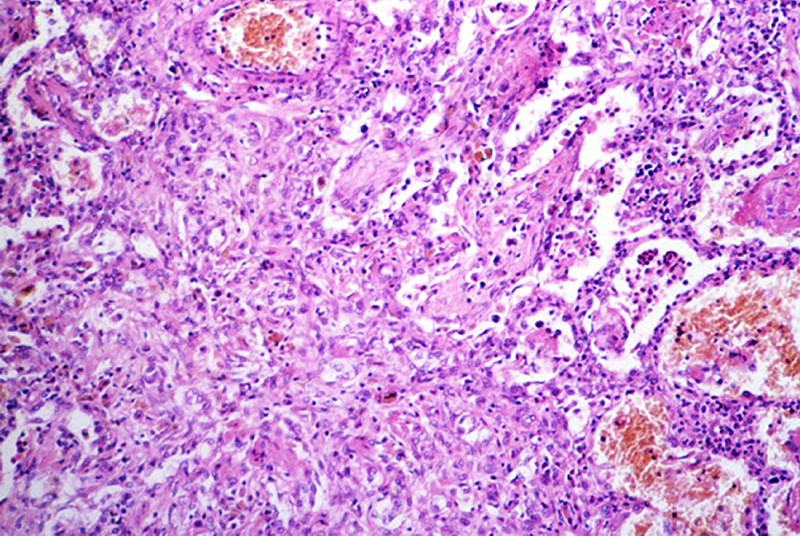
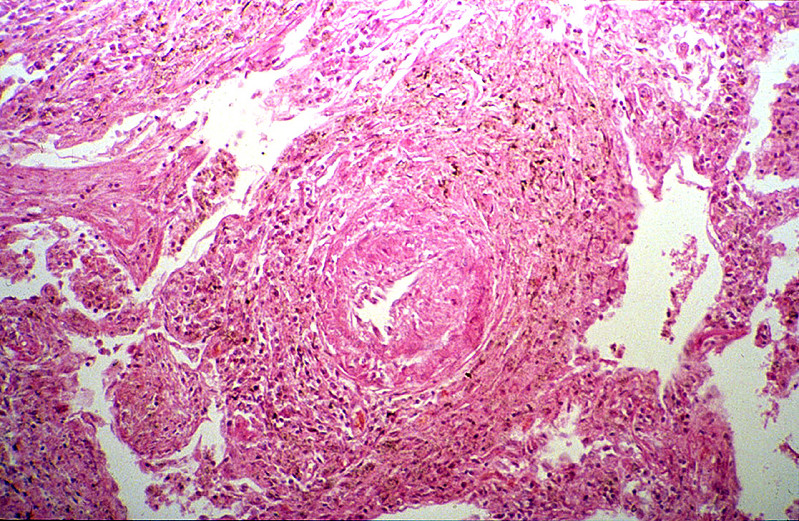
CASE NUMBER 98 Clinical History: This 70-year-old man worked in a rock quarry as a crusher for 18 years. Six months prior to death he began to have dyspnea, orthopnea, paroxysmal nocturnal dyspnea and ankle edema. He was admitted for congestive heart failure and died suddenly with massive pulmonary embolism. Gross: Both lungs were heavy, 900 grams for the left lung and 1120 grams for the right one. The lung was slate gray and firm. Microscopic: In the left upper part of the section the characteristic lesions of silicosis are seen. There are masses of fibrous tissue which form concentric lamination around the blood vessels, and stellate scars when the fibrosis extends to the adjacent alveolar septa. A large amount of coal-black pigment and small crystals are found in the macrophages and the scar tissue. These crystals are best seen under polarized light. In advanced lesion the fibrous nodules become confluent as seen in the lower right part of this section. Notice the presence of arteriosclerosis and organizing thrombi in the pulmonary arteries and chronic inflammation of bronchi. DIAGNOSIS: Silicosis of the Lung Image Gallery:
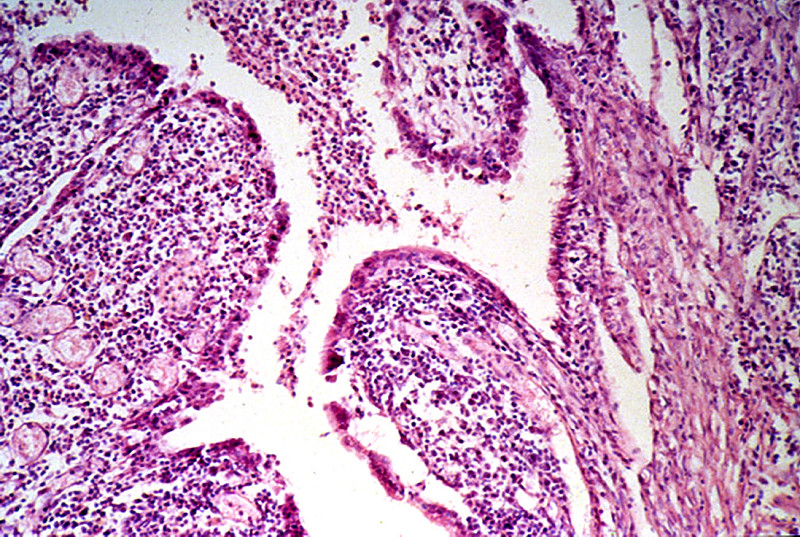
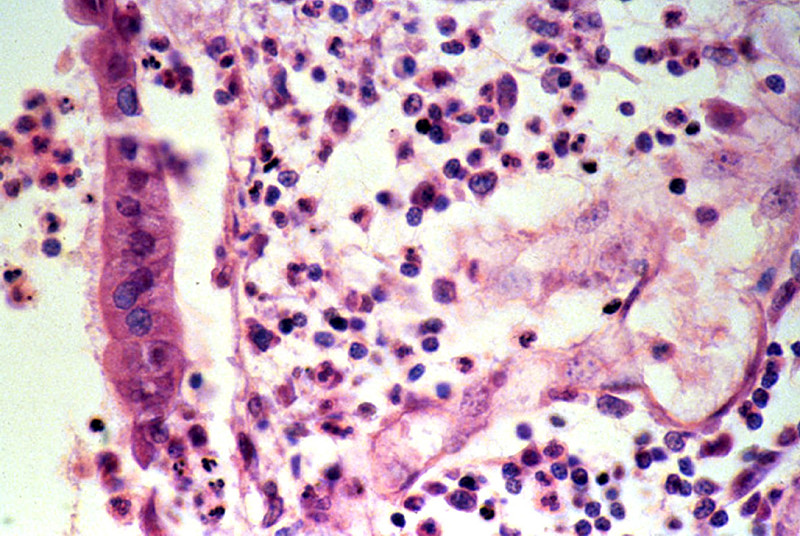
CASE NUMBER 123 Clinical History: A 35-year-old female presented with a five-month history of irregular and prolonged menstrual periods and pelvic pain. The clinical diagnosis was uterine fibroids. Gross: The tubes were markedly distended and thickened with adhesions between the fimbriated end and the ovaries. On sectioning, pus exuded from the lumen. Microscopic: The villi are plump and edematous, with marked dilation and congestion of capillaries. The mucosa is heavily infiltrated by polymorphonuclear leukocytes, which have broken through foci of necrotic mucosa, producing the purulent exudate. Besides this acute phase, there are chronic features evidenced by plasma cell, lymphocytic and macrophage infiltration and fibroblastic proliferation. The muscular layers are edematous and infiltrated by acute and chronic inflammatory cells. This probably represents gonorrheal infection, the mucosa being predominantly involved, in contrast to other pyogenic infections which more frequently involve the outer layers and relatively spare the mucosa. DIAGNOSIS: Acute and Chronic Salpingitis Image Gallery:
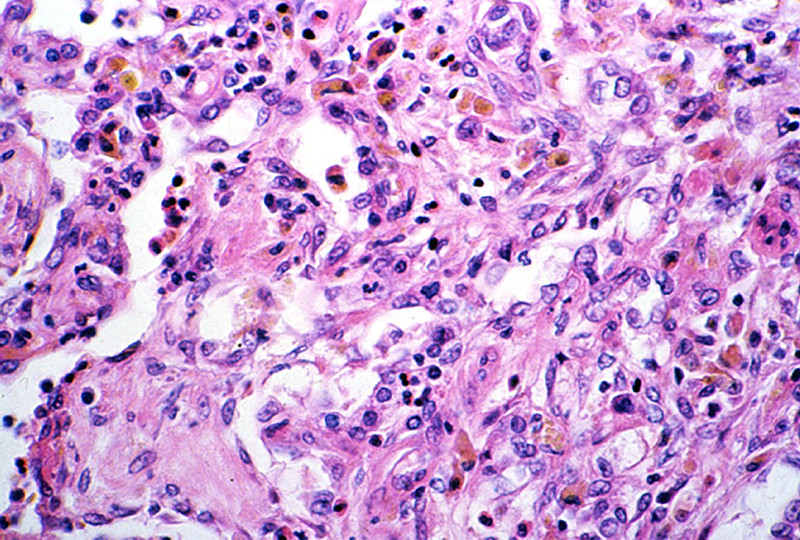
CASE NUMBER 143 Clinical History: This 21-year-old woman had an implant of plastic (etheron) material in her left breast. This was done for cosmetic purposes. The implant caused severe inflammation and had to be removed. Microscopic: The irregular fragments of foreign material are surrounded or engulfed by multinucleated foreign body giant cells. The rest of the section is made up of fibrous connective tissue and collections of lymphocytes and histiocytes. DIAGNOSIS: Foreign Body Reaction Image Gallery:
CASE NUMBER 240 Clinical History: This patient was a 54-year-old male who had a long history of peptic ulcer disease. In this instance both gastric and duodenal ulcers were found. Gross: The gastric mucosa was flattened in most areas, but demonstrated a focal thickening in the area of the ulcer, though no gross ulceration was detected. Microscopic: Microscopic sections show a portion of antral/pyloric stomach. A large ulcer and the accompanying response have replaced all layers of the stomach mucosa and wall. Three layers may be distinguished in the bed of the ulcer. The innermost one is composed of necrotic debris and fibrino-purulent exudate in which bacteria and yeast are present. The middle layer is a zone of granulation tissue made up of small vessels and acute and chronic inflammation. The deepest portion of the ulcer is made up of fibrous scar. Some of the arteries in the scar tissue may show sclerosis. The mucosa adjacent to the ulcer shows acute and chronic gastritis. Helicobacter pylori microorganisms can be discerned overlying the gastric mucosa in some sections. Diagnosis: gastric ulcer Image Gallery:
|
||
Click here to submit questions or comments about this site. Updated 01/14/21 - Velkey |
||