|
|
Cellular Adaptation, Injury & Death Slide list:
Slide Descriptions Slide 1-01. Necrosis, pancreas and fat The underlying cause of necrosis in this tissue is the thrombosis present in the vessel at the lower left of the slide. This has led to coagulative necrosis within pancreatic tissue. Few acini are full-sized. Acini are also disrupted and infiltrated with primarily mononuclear inflammatory cells. Fat necrosis is present at the lower right of the slide. The cell membranes of necrotic adiopcytes are fuzzy, rather than sharply defined. Fat necrosis occurs when injured pancreatic acinar cells release lipolytic enzymes. These enzymes liquefy the adipocyte membranes and release fatty acids from triglycerides. The fatty acids combined with calcium to form insoluble salts that are visible as basophilic deposits on the damaged membranes.
Slide 1-02. Cirrhosis, liver; Pancreas Cirrhosis is defined by 3 characteristics, all of which are well-demonstrated in this section:
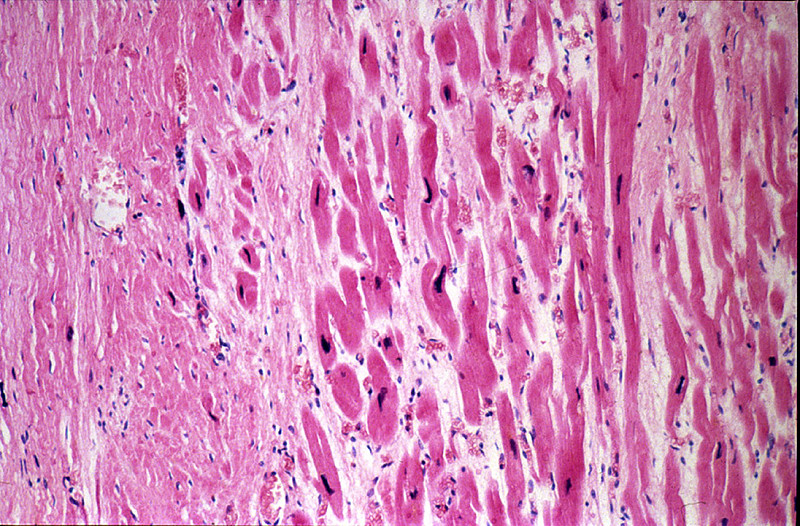
Slide 1-03. Healed myocardial infarct Infarcted myocardial tissue has been replaced by scar tissue (collagen).
Slide 1-04. Recent myocardial infarction Slide 1-04a. Recent myocardial infarction Infarcted muscle fibers (upper left of slide) are surrounded by an inflammatory infiltrate that contains large numbers of neutrophils, dating this infarct to 1-3 days prior to death. Contraction bands are also evident in adjacent tissue. Slide 4a is a duplicate of this slide.
Additional slides from the Duke Medical School Pathology Teaching Collection: CASE NUMBER 14. Acute Tubular Necrosis, Kidney Clinical History: This 37-year-old female ingested about a dozen tablets of mercury bichloride (HgC12). Despite vomiting, treatment with BAL, fluids, and colonic irrigations she became anuric and died 10 days later. The small amount of urine obtained on the first day after taking the pills gave a 4+ benzidine test for occult blood. Gross: The kidneys were both markedly enlarged and pale. Microscopic: The tubular damage here is so severe that it is hard to identify the segment involved. However, it may be noted that most of the necrosis is in the cortex, whereas the collecting tubules in the medulla, although their lumina contain many casts, are lined by relatively intact cells. HgC12 presumably damages mainly proximal convoluted tubules because it is concentrated in this segment. Many involved tubules show marked coagulative necrosis, with sloughing of cells into the lumen. Some tubules that look more nearly normal actually have already have undergone marked necrosis and all that is left is a layer of flattened basilar cells which serve to regenerate the tubule. Regenerative changes can be recognized, including occasional mitoses in epithelial cells. The basement membrane around a few necrotic tubules is broken, and the interstitial tissue contains collections of inflammatory cells and edema fluid. DIAGNOSIS: Acute Tubular Necrosis, Kidney Image Gallery:
CASE NUMBER 31. Recent Myocardial Infarct Clinical History: This 45-year-old man had been well until he was awakened by chest pain that radiated to both arms and neck and was associated with diaphoresis. His blood pressure was 160/110. He was treated with diuretics (Lasix), but despite this he continued to gain weight. Two days after the onset of the chest pain he had a cardiac arrest which was preceded by third degree heart block. Gross: The heart was slightly enlarged weighing 460gms. There was severe atherosclerosis of all the major coronary arteries with a recent thrombotic occlusion of the proximal right coronary artery. A recent transmural infarct was present in the left ventricle that involved the posterior interventricular septum and the posterior papillary muscle. Microscopic: The slide includes a transmural section of the posterior wall of the left ventricle. Nearly the entire section is involved by infarct. However, there is a thin rim (5 to 10 cell layers) of endocardial myocytes which have survived because of diffusion of oxygen and nutrients from the ventricular cavity. Other viable myocytes can be found around larger blood vessels within the section. The intense hypereosinophilia of the necrotic myocytes can best be appreciated by comparing the thin rim of lighter staining subendocardial myocytes with the deeper cells. Note also the karyolysis that is characteristic of coagulation necrosis. In some areas there is little inflammatory response. This observation is explained by microvascular necrosis which does not allow access of circulating leukocytes to these areas. In other areas, especially in the epicardial half of the infarct, there is an intense acute inflammatory response. Many intact neutrophils can be seen. In addition, there are many nuclear fragments from lysed neutrophils. Macrophage activity is not evident. These features of the inflammatory response indicate that the infarct was approximately three to four days old. Note also that the inflammation extends to the epicardial surface and that there are deposits of fibrin on the epicardium. This is called fibrinous pericarditis. The granular grey material seen within some blood vessels is barium sulfate, which was injected to permit post-mortem study of the coronaries by radiography. DIAGNOSIS: Recent Myocardial Infarct Image Gallery:
CASE NUMBER 35. Recent Infarct, Kidney Clinical History: This 76-year-old female was discovered to have a bronchogenic carcinoma six months prior to her death. After a right upper lobectomy she did well, but later developed an "agitated depression". Metastasis to the brain was suspected. Gross: Recent infarcts are seen in Kidneys, Brain, Spleen Microscopic - Kidney: There is recent infarct in this section, with a central area containing "ghosts" of tubules outlined by a marginal zone of polymorphonuclear neutrophils, necrotic debris, and hemorrhage. Some tubules immediately beneath the renal capsule are spared. An artery in the medulla contains a thrombo-embolus that presumably originated from the thrombus on the mitral valve. DIAGNOSIS: Recent Infarct, Kidney Image Gallery:
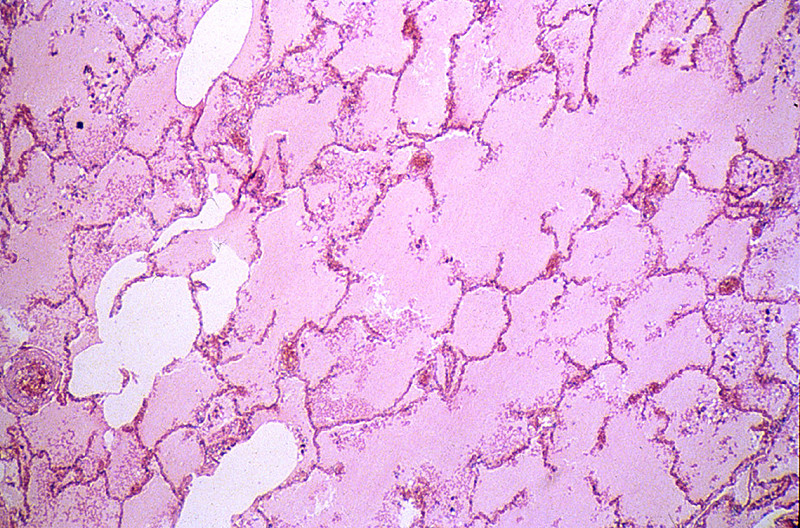
CASE NUMBER 40. Pulmonary Edema Clinical History: A 45-year-old male entered the hospital two days prior to death for evaluation of seizures during the previous month. The neurologic examination was unremarkable. The only symptoms consisted of two seizures. He was found dead by the nurse. Gross: Both lungs were heavy, wet, slightly firm, and dark-red. Microscopic: The alveoli are filled with a homogeneous pink material. The septal capillaries are engorged with blood. An incidental finding consists of anthracotic pigment near the pleural space DIAGNOSIS: Pulmonary Edema Image Gallery:
CASE NUMBER 85. Fatty Liver (lipid accumulation) Clinical History: This 84-year-old female developed weakness and weight loss six months prior to death. She saw a physician twelve days prior to death with signs and symptoms of intestinal obstruction. A tumor mass was palpated in the rectum. She returned home and died with intestinal perforation. She was unable to eat during the last several days of life. Gross: The liver weighed 980 grams. The lobular pattern was accentuated with central areas appearing red and other areas yellow. Microscopic: The areas of fatty change are readily visible with use of scanning power. They are zonal. Note the peri-portal areas are severely involved and the areas of fatty change extend from one portal area to another. The more severely involved cells have eccentric nuclei and the entire cytoplasm is replaced by a fat globule. DIAGNOSIS: Fatty Liver Image Gallery:
CASE NUMBER 95. Hemorrhagic Infarct, Ileum Clinical History: A 60-year-old male had a resection of the right side of colon for adenocarcinoma. Seven days after the operation he had continuous abdominal discomfort and went into shock. A laparotomy revealed that the entire small bowel was gangrenous. Gross: The jejunum and ileum were dark red, thickened and indurated. The mucosal surface was covered by bloody mucus. The cut surface revealed hemorrhages throughout all layers of the intestinal wall. The superior mesenteric vein and its tributaries were obstructed by dark red thrombi which were attached to the vascular wall. Microscopic: The villi are swollen. The superficial layer of the mucosa is necrotic and contains clumps of bacteria. The deeper layer of the mucosa is hemorrhagic but epithelial cells are relatively well preserved. A severe degree of edema, congestion and hemorrhage is seen throughout the submucosa and muscularis layers. The muscle cells are not yet necrotic. DIAGNOSIS: Hemorrhagic Infarct, Ileum Image Gallery:
CASE NUMBER 202. Nodular hyperplasia, prostate Clinical History: A 74-year-old man had hesitancy, intermittency, nocturia, and increasing difficulty in urination for one year. Rectal examination revealed an enlarged, nodular firm prostate. Gross: The prostate was large, nodular, and 120 grams in weight. The capsule was tense, and many gray-white firm nodules bulged out of the cut surface. These nodules varied from 3 mm to 1 cm. The larger ones were present in the lateral lobes and compressed the urethra. Microscopic: Two types of nodules can be distinguished. One is composed essentially of fibro-muscular elements - stromal hyperplasia. The other is composed predominantly of epithelial glands. The size of the glands varies remarkably, and cystic dilatation of some is present. There are two types of cells forming the glands. The lumenal cells are tall columnar cells with basal nuclei and apocrine secretory activity in the cytoplasm. The basal cell layer is composed of cuboidal or flattened epithelium. These glandular nodules are well demarcated by the encircling fibro-muscular stroma. DIAGNOSIS: Nodular Hyperplasia, Prostate Image Gallery:
CASE NUMBER 203. Verruca Vulgaris (hyperplasia) Clinical History: 49-year-old man with lesions on his hands. Gross: There is a 6 mm in diameter gray/tan lesion with a papillated surface. Microscopic: There is marked epidermal hyperplasia with a papillated surface, thickening of the granular layer (hypergranulosis) and cornified layer (hyperkeratosis). Within the granular layer, many of the cells contain large, coarse keratohyalin granules. There are foci of preservation of nuclei in the cornified layer (parakeratosis), especially overlying the tips of the papillae. The vessels in the papillary dermis are dilated. DIAGNOSIS: Verruca Vulgaris Image Gallery:
CASE NUMBER 286. Healed myocardial infarct Clinical History: This 64-year-old male had two episodes of myocardial infarction followed by congestive heart failure during the eight months prior to death. Death was preceded by arrhythmia. Gross: The heart was markedly hypertrophied (740 grams) and dilated. There was marked coronary atherosclerosis with an old occlusion of the left anterior descending vessel. A healed infarct involved the anteroseptal and apical region of the left ventricle. A mural thrombus covered much of the infarct within the heart cavity. Microscopic: The slide includes a transmural section of the anterior free wall and anterior portion of the interventricular septum. There is a broad band of dense, highly collagenized scar tissue replacing the middle layer of myocardium; patchy scarring interspersed with hypertrophied cardiac myocytes is present on either side of this dense scar. The endocardium is markedly thickened and there is organizing mural thrombus between cardiac trabeculae and extending into the lumen. Some myocytes in the subendocardial layer show sarcoplasmic vacuolization, a chronic degenerative change termed "myocytolysis". DIAGNOSIS: Healed myocardial infarct Image Gallery:
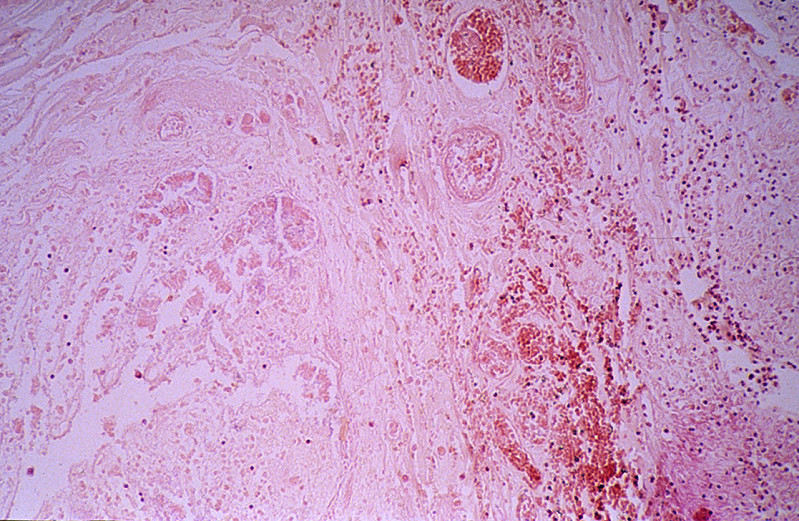
CASE NUMBER 371. Cerebral Infarction Clinical History: The patient was a 67-year-old white female who became disoriented and confused ten days prior to death and developed a weakness on the left side of the body. She had difficulty with vision in the right eye and the retinal artery pressure was decreased on the right. Gross: There was thrombosis of the right internal carotid artery just above the bifurcation. There was extensive necrosis of the right frontal, parietal and temporal lobes and basal ganglia. Microscopic: There is an area of liquefactive necrosis in which many macrophages with phagocytosed fat and myelin particles are present. Around this area are numerous large astrocytes with large vesicular nuclei and abundant eosinophilic cytoplasm. The myelin in this area stains very pale due to surrounding edema fluid. The blood vessels are congested and there is some extravasated blood. DIAGNOSIS: Cerebral Infarction Image Gallery:
CASE NUMBER 429. Hyperplasia, thyroid (colloid nodule) Clinical History: A 50-year-old female had a slowly growing mass in the anterior cervical area for two years. Recent to her admission she had obstruction symptoms and hoarseness. No thyrotoxic manifestations were noted. A subtotal thyroidectomy was performed. Gross: The thyroid was nodular and weighed 250 grams. The capsule was intact. The cut surface revealed large and small honeycombed structures filled with yellow-brown colloid material. Focal hemorrhages and fibrosis were present in the nodules. Microscopic: The nodules consist of small and large follicles up to 3 mm in diameter. The epithelium is low cuboidal, and the colloid is rich. In some sections there is scalloping at the periphery of the colloid. There is fibrosis as well as focal recent and old hemorrhages. A small amount of atrophic, compressed thyroid tissue, may be seen in some sections. DIAGNOSIS: Colloid Nodules of Thyroid (Hyperplastic Thyroid) Image Gallery:
|
||