|
|
Neoplasia Slide list:
Slide Descriptions Slide 6-01. Adenomatous polyp, colon Note the normal appearance of the colon tissue surrounding the lesion, with simple columnar epithelium containing basal nuclei that occupy ~25% of the height of the cell and abundant mucin production. This normal mucosa is present along most of the “stalk” and then transitions abruptly to adenomatous mucosa. The adenomatous changes include nuclear enlargement, such that nuclei occupy 50% or more of the height of the cell. Nuclei are hyperchromatic, have abundant nucleoli, and vary in size from cell to cell. Rather than staying close to the basal portion of the cell, nuclei may be found in the upper portions of the cell (this is loss of polarity). Note the increasingly complex foldings of the adenomatous mucosa compared with normal mucosa. This polyp is classified as demonstrating low grade dysplasia since the complex “gland within a gland” or back to back arrangement of glands characteristic of high grade dysplasia are not present. This polyp is best classified as pre-malignant, neoplastic lesion.
Slide 6-02. Invasive adenocarcinoma of the colon A small focus of normal non-neoplastic mucosa is located on the far right of the slide. The remaining epithelium is neoplastic and located on the surface (in situ) and invading through the wall of the colon. Note the similarity of the cytologic features of the neoplastic cells to those observed in the adenomatous polyp (slide 6-1). Nuclei are enlarged (in most cells they take up more than 50% of the height of the cell), hyperchromatic with multiple nucleoli, vary in size and shape, and lack polarity. Mitotic figures and apoptotic cells are frequent. The invasive neoplastic cells form glands, so this lesion is classified as an adenocarcinoma. Many of the neoplastic glands contain necrotic material with bits of strongly basophilic material in their lumen, the so-called “dirty necrosis” that is characteristic of colon carcinomas. Note the fibrosis that accompanies invasion of the carcinoma into the submucosa (this is called a ‘desmoplastic” response). The pools of mucin containing clusters of the neoplastic cells that produced them that are present in the submucosa are also commonly observed in adenocarcinomas of the colon.
Slide 6-03. Sarcoma, metastatic to lung The nodule of sarcoma dominates the slide, however fairly normal lung tissue can be identified to the right of the slide. The center of the lesion is necrotic (eosinophilic remnants of cell bodies remain, but nuclei are absent) due to tumor growth outstripping its blood supply. The neoplastic cells are spindle-shaped and have some resemblance to smooth muscle cells. Although this tumor is compressing the adjacent lung over most of its perimeter, foci of distinct invasion can be seen at the upper right of the slide.
Slide 6-04. Lung with adenocarcinoma Note the large necrotic center of the tumor nodule. Invasion of the tumor cells into the surrounding lung tissue can be seen in multiple foci. The neoplastic glands are secreting large amounts of mucin.
Slide 6-05. Squamous cell carcinoma of the lung Note the replacement of a portion of the bronchial epithelium with neoplastic squamous cells that invade deeply into the lung parenchyma in the center of the piece of tissue on the right of the slide. The neoplastic cells are present in sheets that somewhat resemble cells present in the skin, with focal secretion of keratin. However, as characteristic of neoplastic cells, the tumor cell nuclei are enlarged, hyperchromatic, and vary in size and shape. There is a desmoplastic response to the presence of tumor, with increased deposition of fibrous tissue adjacent to and between groups of tumor cells.
Slide 6-06. Leiomyoma of the uterus This is a benign smooth muscle tumor that grows and pushes the surrounding tissue out of the way rather than invading. The cells in the leiomyoma very closely resemble their normal counterparts in the surrounding myometrium. However, their abnormal growth has resulted in the grossly apparent mass. Because the smooth muscle cells in this lesion are not incorporated into the rest of the myometrium, leiomyomas impede the contractility of the uterus.
Additional slides from the Duke Medical School teaching collection: CASE NUMBER 5 Clinical History: This 77-year-old male died from pneumococcal meningitis. The patient had a history of advanced tuberculosis, which had been successfully treated, and mild silicosis. Adenocarcinoma of the prostate with several metastases was an unexpected finding. Gross: The prostate was quite large and firm with multiple rubbery nodules measuring 2 mm to 6 mm in diameter. Some of the nodules contain yellowish flecks. The seminal vesicles were firm bilaterally. Microscopic: There are a number of glands shown in varied patterns. In some cases the epithelial cells are found in non-glandular masses. The epithelial cells are cuboidal or polygonal with central, round, deeply pigmented nuclei. Few, if any, mitotic figures can be seen. The presence of perineural and perivascular invasion is clearly in evidence. This is a useful diagnostic characteristic of adenocarcinoma of the prostate. DIAGNOSIS: Adenocarcinoma of Prostate Image Gallery:
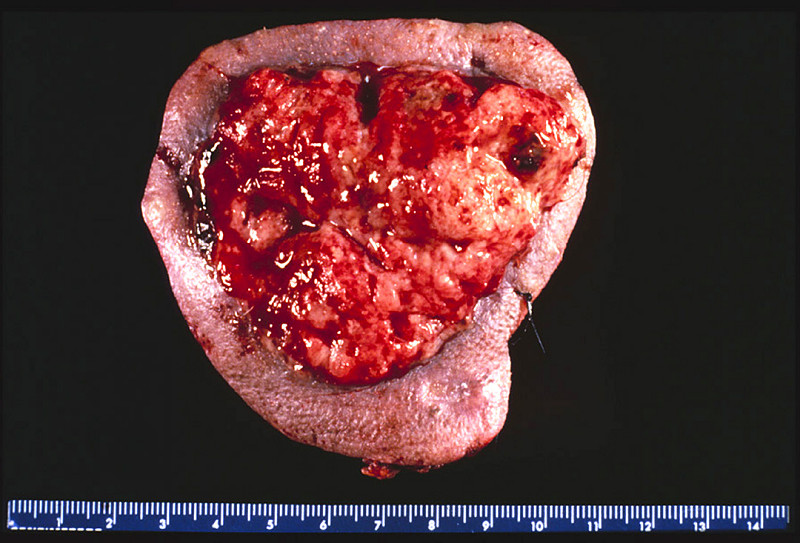
CASE NUMBER 33 Clinical History: This 57-year-old female complained of hematuria. She was cystoscoped and found to have a papillary mass near the dome of the bladder. Microscopic: Orient yourself by naked-eye and low power examination in regard to the 3 main layers of the bladder wall. A normal transitional epithelium lines about 1/2 of the mucosal surface. The central portion is thrown up into many fingerlike fronds (papillae). The connective tissue and vascular core is line by thickened, atypical transitional epithelium. There is a suggestion of very early invasion into the mucosa at the base of the tumor but the muscularis is uninvolved. DIAGNOSIS: Papillary Transitional Cell Carcinoma of Urinary Bladder Image Gallery:
CASE NUMBER 79 Clinical History: A 45-year-old male entered the hospital two days prior to death for evaluation of seizures during the previous month. The neurologic examination was unremarkable. The only symptoms consisted of two seizures. He was found dead by the nurse. Gross: The combined weight of the adrenals was 19 grams. There were several yellow cortical nodules up to 0.6 cm in diameter. Microscopic: Observe without the microscope the nodule of tissue at one end of the section. The cells are mostly in a fascicular arrangement. They are vacuolated and histologically appear identical to normal cortical cells. DIAGNOSIS: Cortical Adenoma, Adrenal Image Gallery:
CASE NUMBER 84 Clinical History: This 84-year-old female developed weakness and weight loss six months prior to death. She saw a physician twelve days prior to death with signs and symptoms of intestinal obstruction. A tumor mass was palpated in the rectum. She returned home and died with intestinal perforation. She was unable to eat during the last several days of life. Gross: The peritoneal cavity contained fecal material. A 1 cm perforation was present in the sigmoid colon. The bowel was markedly distended and filled with fecal material. There were numerous large superficial ulcerations of the large bowel. A tumor was present 4 cm from the anus. It was hard and had completely surrounded the bowel, reducing the lumen to less than 0.5 cm in diameter. Small tumor implants were present over the peritoneum and mesentary nearby. No distant metastases were noted. Microscopic: Inspect the slide first without the microscope. The remainder of the lumen of the bowel can be recognized. Note the thickened bowel wall and masses of tumor surrounding fat. Under low power note the tendency in some areas toward a gland-like structure. There is considerable variation in nuclear staining, size and shape. In some areas clumps of tumor cells are in the midst of mucus which the tumor cells are producing. Note the relatively large amount of dense collagen which accompanies the tumor cells in the fat. DIAGNOSIS: Adenocarcinoma of Rectum Image Gallery:
CASE NUMBER 134 Clinical History: An 81-year-old, otherwise asymptomatic female was found to have guaiac-positive stool on routine examination. Flexible sigmoidoscopy revealed a rectal mass. Gross: A 5 cm fungating, centrally ulcerated mass was found on gross examination. Microscopic: This section, which includes the edge of the tumor shows invasive adenocarcinoma arising in a villous adenoma. Tall villi lined by neoplastic epithelium replace the normal mucosa at the edge of the mass. Centrally, where the lesion was ulcerated, tumor infiltrates through the muscularis propria and in some sections, enters the subserosal adipose tissue. Irregular glandular spaces are lined by tumor cells and large pools of mucin are seen, as well as desmoplastic (fibrotic) stroma. Although the nuclei of the carcinoma are anaplastic when compared to the normal colon mucosa, the neoplastic epithelium retains a columnar appearance, typically seen in colon carcinoma. DIAGNOSIS: Adenocarcinoma of Colon
CASE NUMBER 139 Clinical History: A 68-year-old man was found to have guaiac-positive stools. Colonoscopy revealed a sigmoid colon mass. Elevated liver function tests raised the suspicion of metastases and CT scan showed a liver mass. The colon primary was resected and a partial hepatectomy was performed. Gross: An 8 cm area of liver was replaced by a tumor mass. The tumor was firm and white in comparison to the surrounding soft, golden brown liver. Areas of hemorrhage and necrosis could be seen within the tumor. Microscopic: A small portion of residual liver can be seen in most sections. The tumor mass is made up of irregular glandular spaces lined by malignant, cuboidal to columnar epithelium. The neoplastic glands are dispersed in desmoplastic (fibrotic) stroma. DIAGNOSIS: Metastatic Colon Carcinoma in Liver Image Gallery:
CASE NUMBER 154 Clinical History: A 64-year-old man complained of hoarseness and throat pain. Gross: A tumor involved the right true and false vocal cord and extended across the midline. Microscopic: The mucosa is partially columnar, representing the ventricular mucosa. There is a transition to squamous mucosa with marked nuclear pleomorphism. The abnormal squamous cells extend into the underlying stroma where the cells keratinize. Focal necrosis and an inflammatory infiltrate is present. DIAGNOSIS Squamous Cell Carcinoma of the Larynx Image Gallery:
CASE NUMBER 155 Clinical History: A 62-year-old male died of bronchopneumonia. He was an alcoholic and ate poorly for many years. Gross: In the right lobe of the liver there was a circumscribed, dark red, spongy mass 4 cm in size. In the center of the mass there was a gray, firm, fibrous core. Microscopic: Naked eye inspection reveals a mass with many blood filled spaces. These are formed by anastomosing strands of connective tissue, partially hyalinized, lined by endothelial cells. Notice the subcapsular location of the tumor and its relationship to the liver parenchyma. DIAGNOSIS: Cavernous Hemangioma of Liver Image Gallery:
CASE NUMBER 166 Clinical History: A 43-year-old female had a four-month history of intermittent bloody stools. Sigmoidoscopy revealed pedunculated polyps 15 cm above the sphincter. Gross: The resected tissue was a double stalked and double headed polyp of 1.5 cm in diameter. The stalk was 2 cm in length. The base of the stalk and the adjacent mucosa showed no induration. Microscopic: The exophytic structure of the polyp can be seen with the naked eye. There is a short stalk lined by normal colon mucosa with blood vessels in the submucosa. The finger-like villi of the polyp are lined by adenomatous mucosa, the hallmark of a neoplastic polyp. Compared to the nearby normal mucosa, the nuclei are elongated, hyperchromatic and stratified. There is increased nuclear to cytoplasmic ratio and decreased cytoplasmic mucin. DIAGNOSIS: Tubulovillous Adenoma (Polyp) of Colon Image Gallery:
CASE NUMBER 170 Clinical History: This was an incidental finding in the lung in a case of uremia due to chronic pyelonephritis in a 67-year-old male. Gross: There was a hard, very well circumscribed, round nodule with a greyish glassy cut surface in the lung. Microscopic: There is normal cartilage, hyperplastic bronchial epithelium, and fragments of lung tissue with the alveoli filled with mononuclear cells derived from the alveolar epithelial cells. These lesions are common and seldom cause clinical symptoms. DIAGNOSIS: Cartilaginous Hamartoma Image Gallery:
CASE NUMBER 199 (slide 033_ZZ) Clinical History: A 34-year-old woman discovered a mass in her breast. Gross: A 3 x 3 x 2 cm firm mass was found in the breast. Microscopic: Ductal carcinomas range from well-differentiated tumors characterized by good duct formation to poorly-differentiated tumors such as this one which is composed of sheets of pleomorphic cells which infiltrate into the adjacent breast tissue. This tumor also has evoked a strong lymphocytic response. A special form of breast cancer, referred to as medullary carcinoma, is also poorly-differentiated with an abundant lymphocytic response, but it is well-circumscribed and has a better prognosis than this tumor. Also note the adjacent normal breast lobules. In some there is also a lymphocytic infiltrate, though no tumor is seen in them. DIAGNOSIS: Infiltrating Ductal Carcinoma of the Breast Image Gallery:
CASE NUMBER 220 Clinical History: This was a 58-year-old female whose uterus was removed along with the ovaries for an ovarian teratoma. Gross: The uterus was slightly enlarged, and contained many gray firm circumscribed nodules 0.5 cm - 2 cm in size. These nodules bulged out of the cut surface. Most of them were located intramurally, but there were some submucously and subserously located. Microscopic: The tumor nodules are composed of interlacing bundles of cells, which have long spindle nuclei and pink fibrillary cytoplasm. These cells resemble the smooth muscle cells of the myometrium. Portions of the tumor tissue have become pink hyalinized masses in which only a few cells are present. These tumor nodules do not have a definite capsule, though their outlines are rather distinct. A small number of vessels are present within the tumor. DIAGNOSIS: Leiomyoma of Uterus Image Gallery:
CASE NUMBER 223 Clinical History: A 13-year-old male had an enlarging mass in the left thigh for 1 1/2 months. It was not associated with pain or tenderness. The X-ray revealed a large tumor extending around the entire shaft and lower 1/3 or the left femur. Amputation was performed after biopsy. Gross: The tumor was a large, pink-gray, soft and granular mass, 8x4x5 cm in size, involving the lower femoral shaft, and growing into the muscle. Microscopic: The tumor is composed of sheaths of loosely packed fibroblastic and osteoblastic cells, which have large hyperchromatic nuclei and scanty eosinophilic cytoplasm. In the intercellular spaces of the tumor there is deposition of pink homogeneous osteoid tissue which frequently transforms into irregular, bony trabeculae. New periosteal bone formation may be seen in the section. DIAGNOSIS: Osteogenic Sarcoma of Bone Image Gallery:
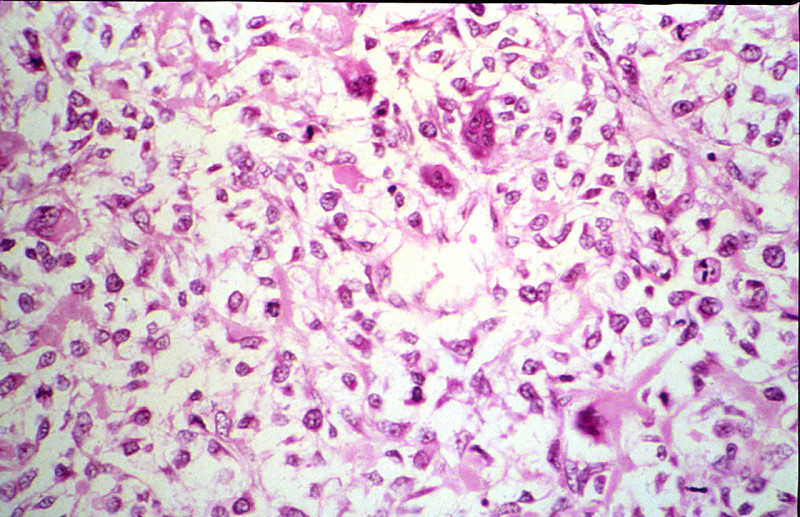
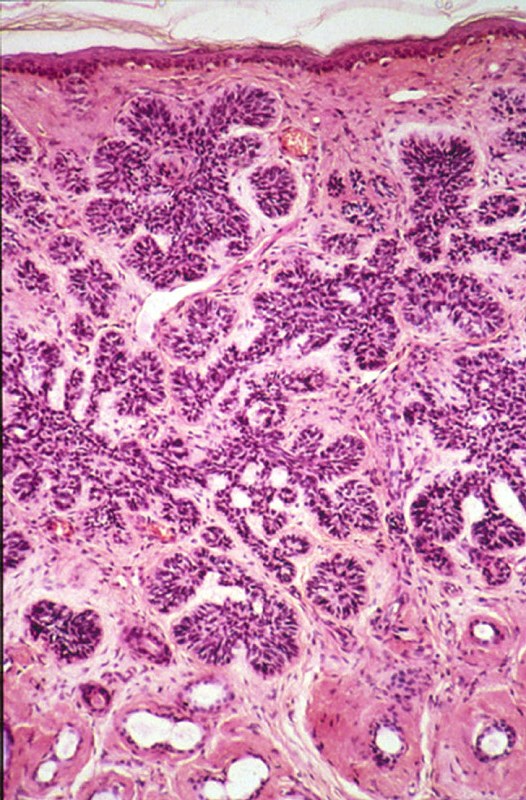
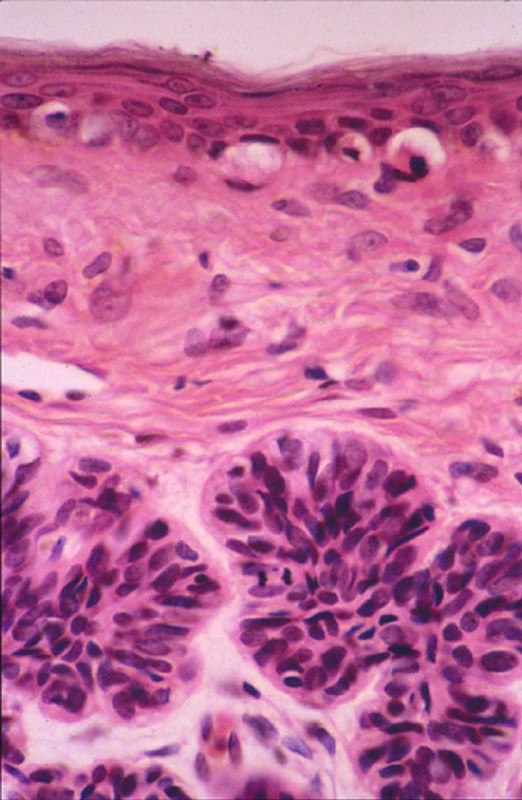
CASE NUMBER 227 Clinical History: A 62-year-old male entered with a complaint of a lesion on the right cheek of eight months duration. It had been growing slowly. Gross: There was a well circumscribed, firm, elevated mass 1 cm in diameter. The overlying skin was intact but smooth and somewhat dark colored. Microscopic: There are nests of darkly staining basophilic cells in the upper dermis with peripheral palisading. There is little cytoplasm, and the cytoplasmic borders are poorly defined. Nuclei are small and are round or oval, and occasional apoptotic bodies are noted. These tumors may arise from the basal cell layer of the epidermis or from dermal appendages. In this particular tumor there is an occasional round mass of keratin which is not usually seen in basal cell carcinomas. Note the loose, myxoid stroma about the tumor cells with some artifactual clefts. DIAGNOSIS: Basal Cell Carcinoma Image Gallery:
CASE NUMBER 253 Clinical History: A 60-year-old female had a one year history of weight loss and upper gastro-intestinal obstruction for three months. Gross: The resected portion of the stomach showed a large fungating, partially ulcerated tumor mass in the antrum. Regional lymph nodes and a liver biopsy were free of tumor. Microscopic: There is a rather abrupt change of the normal stomach mucosa to malignant tumor tissue, projecting into the lumen as a cauliflower-like mass. The tumor forms abundant irregular acini, lined by one or more layers of atypical cells with mostly large irregular nuclei and poorly defined eosinophilic cytoplasm. Atypical mitoses are moderately frequent. The tumor has infiltrated through the muscularis mucosa and the edematous submucosa and has invaded the muscle layers. The invading tumor had elicited a rather marked neutrophilic and plasma cell response. DIAGNOSIS: Adenocarcinoma of Stomach (Intestinal Type) Image Gallery:
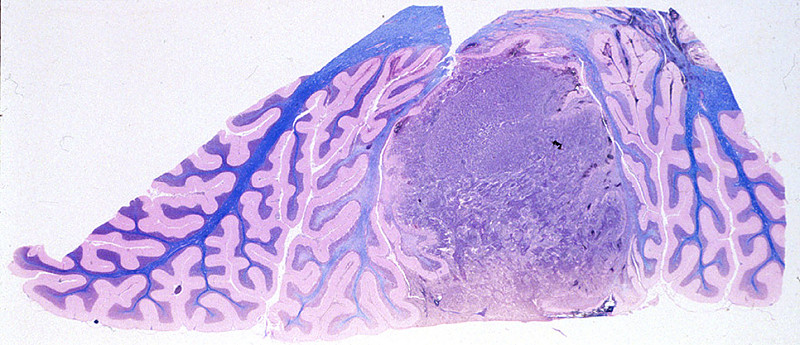
CASE NUMBER 329 Clinical History: This 16-year-old female had a four month history of headache. She developed seizures one week prior to death and was found to have a coarse vertical nystagmus and papilledema. At surgery, a posterior fossa tumor was found. Gross: A medulloblastoma was found in the anterior mid-cerebellum and extending laterally into the right lobe. It measured 2xIx1 cm. There was some tumor infiltration into the dentate nucleus. Microscopic: The section shows cerebellum with a pink molecular layer. Underlying that is the Purkinje cell layer composed of lage pyramidal neurons. Next is the granular cell layer. Granule cells are neurons. They are the cell on origin of medulloblastoma. Not the similar appearance to the tumor cells. The tumor consists of cells with round or oval dark staining nuceli. Mitotic figures are present. The white matter of the cerebellum stains blue with the luxol fast blue stain. (Luxol Fast Blue - H&E stain) DIAGNOSIS: Medulloblastoma Image Gallery:
CASE NUMBER 427 Clinical History: A 78-year-old male was admitted with headache and bitemporal hemianopsia of several years duration. No endocrine disturbances were noted. Gross: The pituitary gland, weighing 3gms and measuring 2 cms in greatest diameter, contained a large pink-gray soft tumor mass in the anterior lobe. The optic chiasm was slightly atrophic due to the compression of the tumor. Microscopic: The tumor occupies nearly the entire anterior lobe, so that only a thin rim of normal hypophyseal tissue is present in the subcapsular area. The tumor is composed of uniform cells arranged in a trabecular or sinusoidal pattern. The stroma is highly vascular. Some of the tumor cells contain fine eosinophilic granules, but most of them are chromophobes with special stains. DIAGNOSIS: Chromophobe Adenoma, Pituitary Image Gallery:
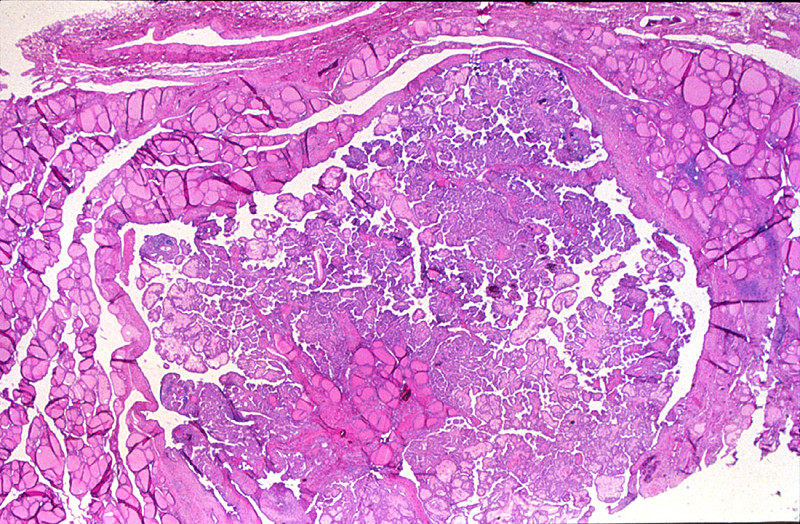
CASE NUMBER 430 Clinical History: A 23-year-old man presented with a nodule in his neck. Gross: The patient was found to have an enlarged lymph node and a thyroid nodule. Microscopic: The lesions in the lymph node and thyroid are similar. The tumor is composed of papillae covered by closely packed cells with bland, sometimes optically-clear ("Orphan-Annie eye") nuclei. Nuclear grooves are also present. A few round purplish calcifications, termed psammoma bodies, are also seen. DIAGNOSIS: Papillary Carcinoma of the Thyroid Image Gallery:
|
||