|
|
Hemodynamic and Vascular Disorders Slide list:
Slide Descriptions Slide 3-01. Atherosclerosis, coronary artery The slide contains 4 cross-sections of coronary artery that demonstrate varying degrees of lipid accumulation in the intima and calcification.
Slide 3-02. Pulmonary embolism, lung Both sections of lung contain occlusive emboli in a large branch of the pulmonary artery.
Slide 3-03. Infarct, spleen
Slide 3-04. Coagulative necrosis, liver The necrosis occurs in a centrilobular pattern, with necrotic tissue present surrounding the central vein. This is the pattern typically observed when the liver experiences ischemia. The periportal areas are relatively preserved since oxygen levels are highest there.
Slide 3-05. Thrombosis, periprostatic veins Note the laminar (many layered) nature of the clot and its adhesion to the vessel wall.
Slide 3-06. Thromboembolus in an atherosclerotic vessel, lung Numerous macrophages filled with the golden-brown pigment hemosiderin are present within the alveoli. Cholesterol clefts are prominent in the media of the atherosclerotic vessel. A longitudinal section of embolus attached to the pulmonary artery is also present on the section.
Slide 3-07. Hemorrhage and infarction, lung Most of the alveoli contain numerous red blood cells. Several foci of hemorrhagic infarction are present. In these areas, the outlines of the alveoli can still be discerned but the alveolar epithelial cells have experienced karyolysis. This is an example of coagulative necrosis due to infarction.
Slide 3-08. Multiple pulmonary emboli, lungs Thromboemboli are present in many small and medium-sized vessels in all 3 sections of the lung.
Additional slides from the Duke Medical School Pathology Teaching Collection: CASE NUMBER 14. Acute Tubular Necrosis, Kidney Clinical History: This 37-year-old female ingested about a dozen tablets of mercury bichloride (HgC12). Despite vomiting, treatment with BAL, fluids, and colonic irrigations she became anuric and died 10 days later. The small amount of urine obtained on the first day after taking the pills gave a 4+ benzidine test for occult blood. Gross: The kidneys were both markedly enlarged and pale. Microscopic: The tubular damage here is so severe that it is hard to identify the segment involved. However, it may be noted that most of the necrosis is in the cortex, whereas the collecting tubules in the medulla, although their lumina contain many casts, are lined by relatively intact cells. HgC12 presumably damages mainly proximal convoluted tubules because it is concentrated in this segment. Many involved tubules show marked coagulative necrosis, with sloughing of cells into the lumen. Some tubules that look more nearly normal actually have already have undergone marked necrosis and all that is left is a layer of flattened basilar cells which serve to regenerate the tubule. Regenerative changes can be recognized, including occasional mitoses in epithelial cells. The basement membrane around a few necrotic tubules is broken, and the interstitial tissue contains collections of inflammatory cells and edema fluid. DIAGNOSIS: Acute Tubular Necrosis, Kidney Image Gallery:
CASE NUMBER 28 Clinical History: A 47-year-old female with a history of hypertension of at least 8 months duration noted sudden onset of severe inter-scapular pain which rapidly radiated to base of neck but not to abdomen 7 hours prior to admission. On admission her BP was 160/130 (both arms) and pulse was 80 and equal bilaterally. No murmurs were noted. A retrograde aortogram revealed a double channel extending from the root of the aorta to the innominate artery. Aortotomy was performed for attempted repair of the dissecting aneurysm, but during the procedure there occurred an adventitial tear with subsequent hemopericardium and cardiac tamponade. The patient expired on the operating table 6 hours after surgery had begun. Gross: The heart weight was 550 grams and there was left ventricular hypertrophy. The aorta had an intimal tear at the base of the innominate artery with dissection of the media occurring in the outer 2/3 and extending proximally to within 0.5 cm of the aortic valve. There was an adventitial tear at this point. Microscopic: There is a blood-filled tear between the inner 2/3 and outer 1/3 of the media. Note necrosis and deposition of fibrin along the margins of the defect. The remainder of the media contains the changes of "cystic medial necrosis" DIAGNOSIS: Dissecting Aneurysm, Ascending Aorta, with cystic medial necrosis Image Gallery:
CASE NUMBER 31. Recent Myocardial Infarct Clinical History: This 45-year-old man had been well until he was awakened by chest pain that radiated to both arms and neck and was associated with diaphoresis. His blood pressure was 160/110. He was treated with diuretics (Lasix), but despite this he continued to gain weight. Two days after the onset of the chest pain he had a cardiac arrest which was preceded by third degree heart block. Gross: The heart was slightly enlarged weighing 460gms. There was severe atherosclerosis of all the major coronary arteries with a recent thrombotic occlusion of the proximal right coronary artery. A recent transmural infarct was present in the left ventricle that involved the posterior interventricular septum and the posterior papillary muscle. Microscopic: The slide includes a transmural section of the posterior wall of the left ventricle. Nearly the entire section is involved by infarct. However, there is a thin rim (5 to 10 cell layers) of endocardial myocytes which have survived because of diffusion of oxygen and nutrients from the ventricular cavity. Other viable myocytes can be found around larger blood vessels within the section. The intense hypereosinophilia of the necrotic myocytes can best be appreciated by comparing the thin rim of lighter staining subendocardial myocytes with the deeper cells. Note also the karyolysis that is characteristic of coagulation necrosis. In some areas there is little inflammatory response. This observation is explained by microvascular necrosis which does not allow access of circulating leukocytes to these areas. In other areas, especially in the epicardial half of the infarct, there is an intense acute inflammatory response. Many intact neutrophils can be seen. In addition, there are many nuclear fragments from lysed neutrophils. Macrophage activity is not evident. These features of the inflammatory response indicate that the infarct was approximately three to four days old. Note also that the inflammation extends to the epicardial surface and that there are deposits of fibrin on the epicardium. This is called fibrinous pericarditis. The granular grey material seen within some blood vessels is barium sulfate, which was injected to permit post-mortem study of the coronaries by radiography. DIAGNOSIS: Recent Myocardial Infarct Image Gallery:
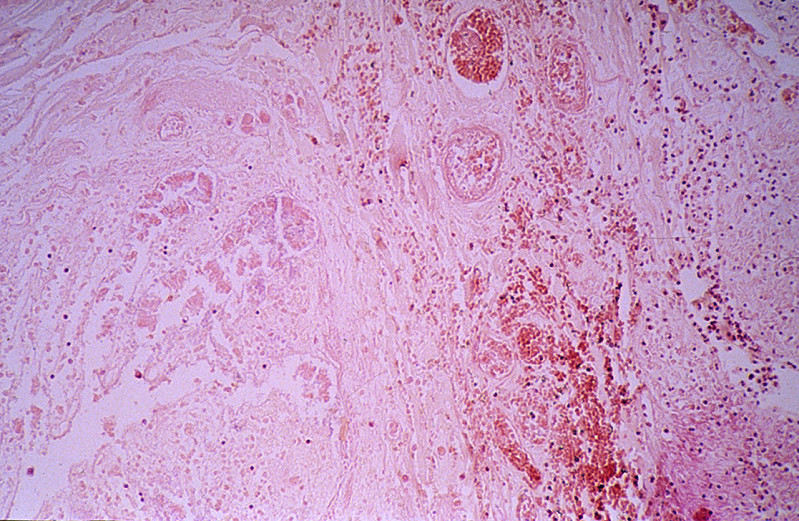
CASE NUMBER 35. Recent Infarct, Kidney Clinical History: This 76-year-old female was discovered to have a bronchogenic carcinoma six months prior to her death. After a right upper lobectomy she did well, but later developed an "agitated depression". Metastasis to the brain was suspected. Gross: Recent infarcts are seen in Kidneys, Brain, Spleen Microscopic - Kidney: There is recent infarct in this section, with a central area containing "ghosts" of tubules outlined by a marginal zone of polymorphonuclear neutrophils, necrotic debris, and hemorrhage. Some tubules immediately beneath the renal capsule are spared. An artery in the medulla contains a thrombo-embolus that presumably originated from the thrombus on the mitral valve. DIAGNOSIS: Recent Infarct, Kidney Image Gallery:
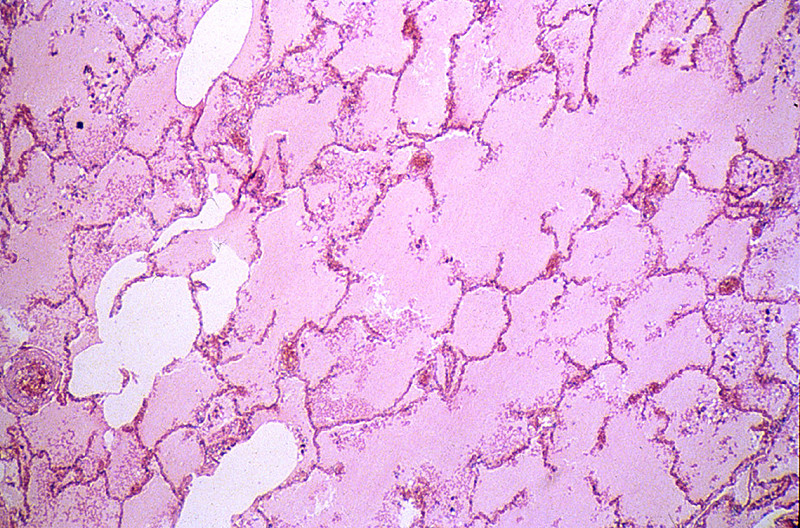
CASE NUMBER 40. Pulmonary Edema Clinical History: A 45-year-old male entered the hospital two days prior to death for evaluation of seizures during the previous month. The neurologic examination was unremarkable. The only symptoms consisted of two seizures. He was found dead by the nurse. Gross: Both lungs were heavy, wet, slightly firm, and dark-red. Microscopic: The alveoli are filled with a homogeneous pink material. The septal capillaries are engorged with blood. An incidental finding consists of anthracotic pigment near the pleural space DIAGNOSIS: Pulmonary Edema Image Gallery:
CASE NUMBER 95. Hemorrhagic Infarct, Ileum Clinical History: A 60-year-old male had a resection of the right side of colon for adenocarcinoma. Seven days after the operation he had continuous abdominal discomfort and went into shock. A laparotomy revealed that the entire small bowel was gangrenous. Gross: The jejunum and ileum were dark red, thickened and indurated. The mucosal surface was covered by bloody mucus. The cut surface revealed hemorrhages throughout all layers of the intestinal wall. The superior mesenteric vein and its tributaries were obstructed by dark red thrombi which were attached to the vascular wall. Microscopic: The villi are swollen. The superficial layer of the mucosa is necrotic and contains clumps of bacteria. The deeper layer of the mucosa is hemorrhagic but epithelial cells are relatively well preserved. A severe degree of edema, congestion and hemorrhage is seen throughout the submucosa and muscularis layers. The muscle cells are not yet necrotic. DIAGNOSIS: Hemorrhagic Infarct, Ileum Image Gallery:
CASE NUMBER 158 Clinical History: A 63-year-old male had a five year history of progressive weakness and congestive heart failure. Gross: The left lung was dark red and heavy, and a large amount of hemorrhagic frothy fluid exuded freely from the cut surface. In the main pulmonary artery there was a large red firm clot adherent to the vascular wall. Many small blood clots were present in the vessels of the upper and lower lobes. Associated with these were many wedge-shaped, dark red, firmer areas in the lung parenchyma. Microscopic: There are two sections of most slides. On one slide there are organizing thrombi in the pulmonary arteries. On the other side there is a large hemorrhagic area in which some alveolar septa are pink, smudgy, and necrotic. In other portions of the lung the septa are thickened with fibrosis. DIAGNOSIS: Pulmonary Embolism and Hemorrhagic Infarct Image Gallery:
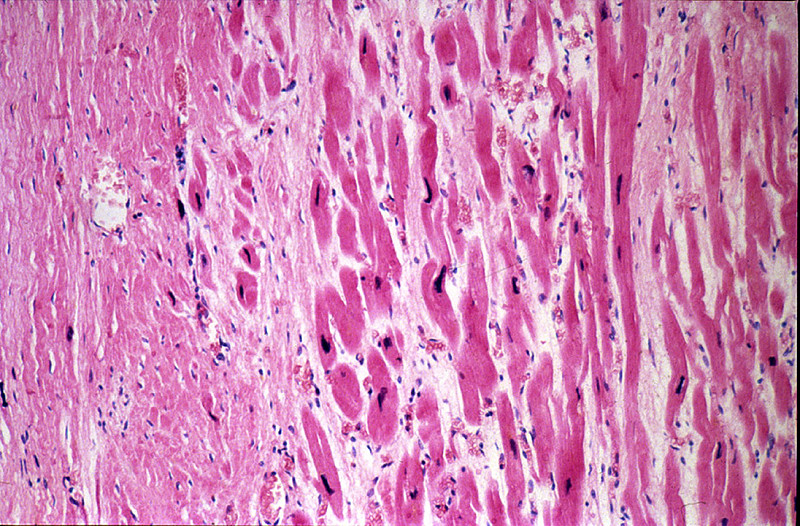
CASE NUMBER 286. Healed myocardial infarct Clinical History: This 64-year-old male had two episodes of myocardial infarction followed by congestive heart failure during the eight months prior to death. Death was preceded by arrhythmia. Gross: The heart was markedly hypertrophied (740 grams) and dilated. There was marked coronary atherosclerosis with an old occlusion of the left anterior descending vessel. A healed infarct involved the anteroseptal and apical region of the left ventricle. A mural thrombus covered much of the infarct within the heart cavity. Microscopic: The slide includes a transmural section of the anterior free wall and anterior portion of the interventricular septum. There is a broad band of dense, highly collagenized scar tissue replacing the middle layer of myocardium; patchy scarring interspersed with hypertrophied cardiac myocytes is present on either side of this dense scar. The endocardium is markedly thickened and there is organizing mural thrombus between cardiac trabeculae and extending into the lumen. Some myocytes in the subendocardial layer show sarcoplasmic vacuolization, a chronic degenerative change termed "myocytolysis". DIAGNOSIS: Healed myocardial infarct Image Gallery:
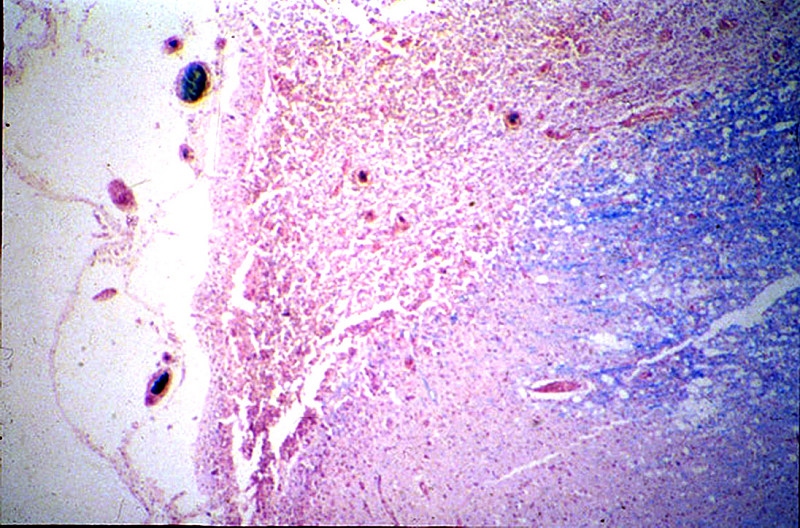
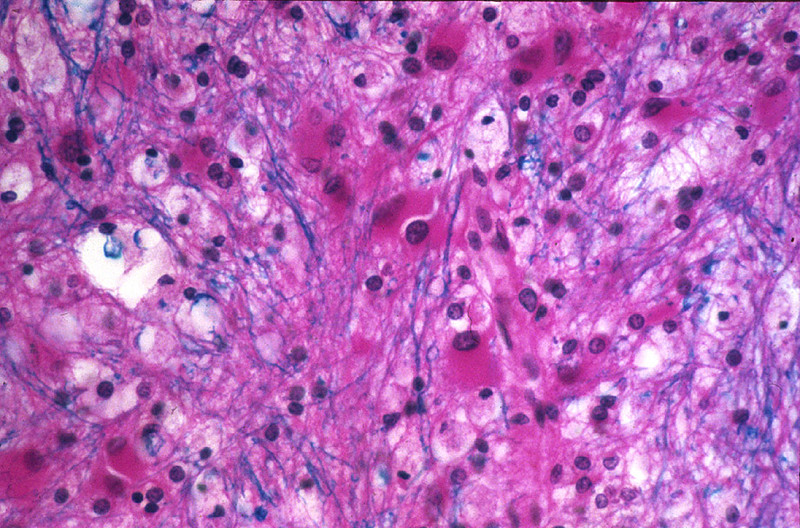
CASE NUMBER 370 Clinical History: The patient was a 67-year-old female who became disoriented and confused ten days prior to death and developed clumsiness on the left side of the body. She had vertigo (sensation of the room spinning) and a leftward-beating nystagmus (eyes drifting slowly to her right and then quickly darting back to her left). Her left eyelid drooped (ptosis) and her left pupil was constricted (miosis). A sensory exam showed loss of pain sensation on the right side of her body (limbs and trunk) and the left side of her face. Gross: There was thrombosis of the posterior inferior cerebellar artery (PICA). There was extensive necrosis of the left posterior, inferior cerebellum and left lateral anterior medulla. Microscopic: There are areas of liquefactive necrosis in the cerebellum and lateral medulla. Around these areas are some large astrocytes with large vesicular nuclei and abundant eosinophilic cytoplasm. The myelin in these areas stains very pale due to surrounding edema fluid. The blood vessels are congested and there is some extravasated blood. (Luxol Fast Blue - H&E stain) DIAGNOSIS: Infarct of Cerebellum and Lateral Medulla of the Brainstem Image Gallery:
CASE NUMBER 371. Cerebral Infarction Clinical History: The patient was a 67-year-old white female who became disoriented and confused ten days prior to death and developed a weakness on the left side of the body. She had difficulty with vision in the right eye and the retinal artery pressure was decreased on the right. Gross: There was thrombosis of the right internal carotid artery just above the bifurcation. There was extensive necrosis of the right frontal, parietal and temporal lobes and basal ganglia (the gross image is a posterior view of a coronal slice, so the right side of the image is the anatomical right). Microscopic: There is an area of liquefactive necrosis in which many macrophages with phagocytosed fat and myelin particles are present. Around this area are numerous large astrocytes with large vesicular nuclei and abundant eosinophilic cytoplasm. The myelin in this area stains very pale due to surrounding edema fluid. The blood vessels are congested and there is some extravasated blood. DIAGNOSIS: Cerebral Infarction Image Gallery:
|
||