|
|
Duke Pathology 200 Comprehensive Slide List
(click here to SHOW diagnoses) or (click here to HIDE diagnoses)
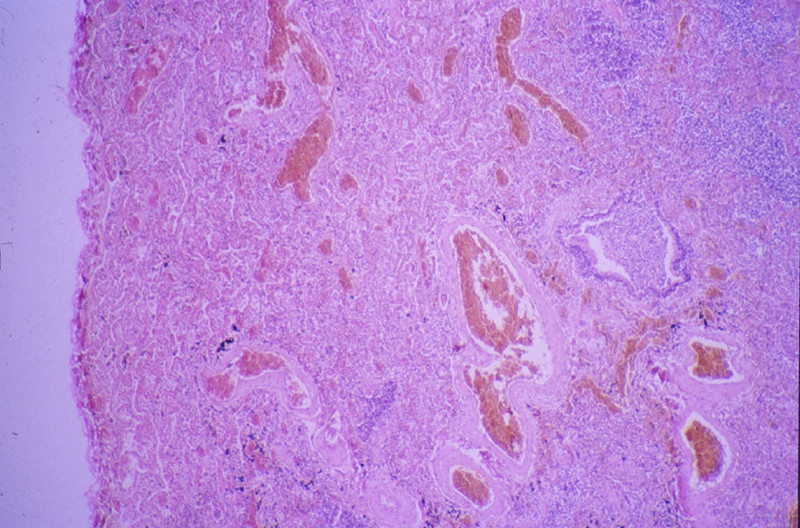
Slide Descriptions CASE NUMBER 1 Clinical History: This 15-day-old female child had multiple congenital cardiac defects. In addition, bilateral abdominal masses were present. Microscopic: This is a complete hemisection of the kidney. Examination with naked eye or inverted ocular reveals that the entire kidney has a honeycombed appearance. Microscopic examination shows the cysts to be markedly dilated tubules that contain granular eosinophilic material (probably protein) and in some cases, red blood cells. The glomeruli, in contrast to those of an adult kidney, contain peripheral rows of visceral epithelial cells. This pattern, which disappears during the course of several years, is normal for infant glomeruli. Polycystic renal disease may also present in adulthood, in which case the kidneys are often grossly enlarged and virtually replaced by cysts up to several centimeters in diameter. DIAGNOSIS: Polycystic Kidney Image Gallery:
CASE NUMBER 2 Clinical History: This 45 year man noticed blood in his urine. His physician ordered a CT of the lower abdomen and pelvis. A mass in the superior pole of the kidney was discovered. A biopsy was performed and then the kidney was removed. Gross: There is a large yellow tan tumor with areas of hemorrhage in the superior pole of the kidney. The tumor invades the renal vein and the perinephric adipose tissue. Microscopic: The capsule is revealed to be actually a pseudo capsule formed by compression of surrounding renal parenchyma. The tumor is made up mainly of large irregular cells, some with granular cytoplasm, and others with large vacuoles. The nuclei vary in size and shape. Some are pyknotic and some are displaced to the periphery of the large vacuolated cells characteristic of this disease. DIAGNOSIS: Renal cell carcinoma Image Gallery:
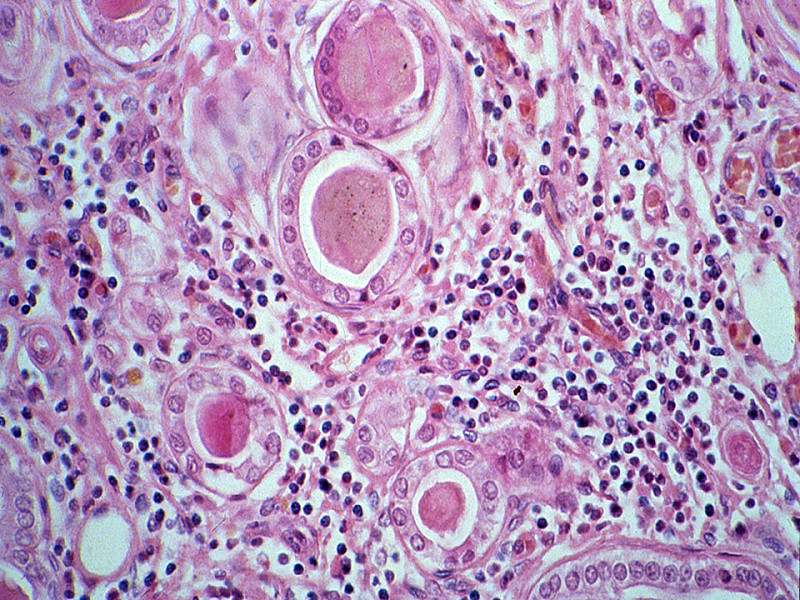
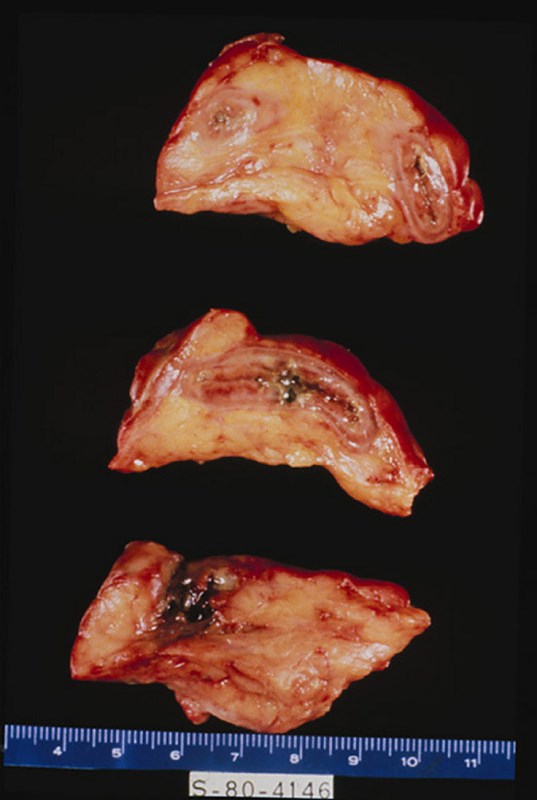
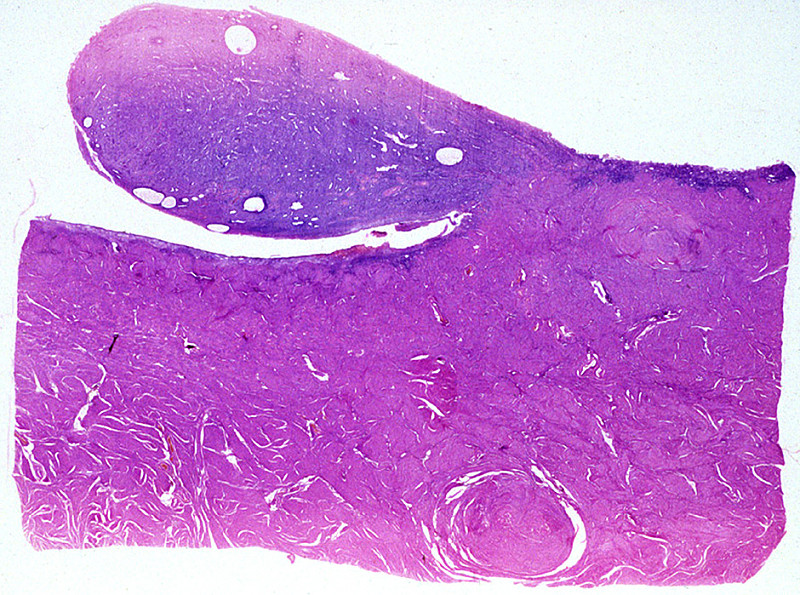
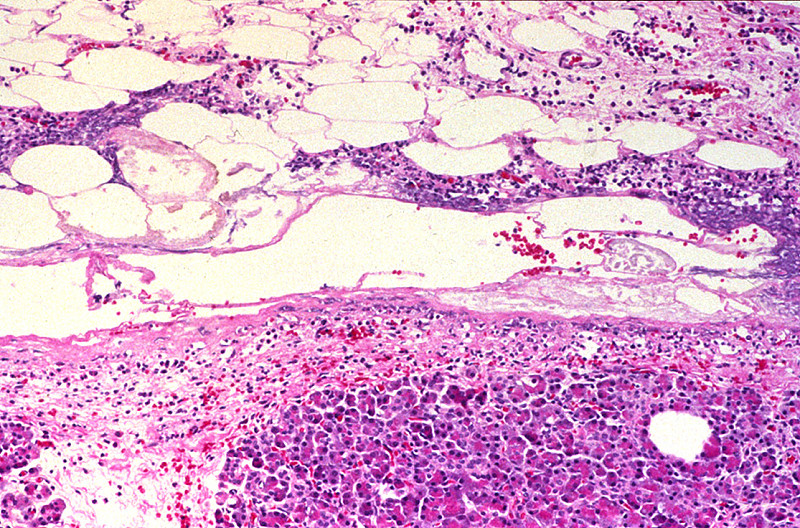
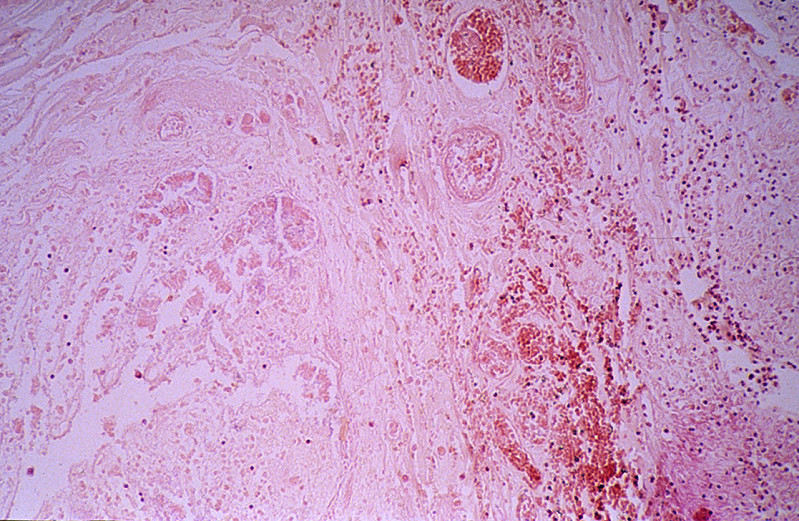
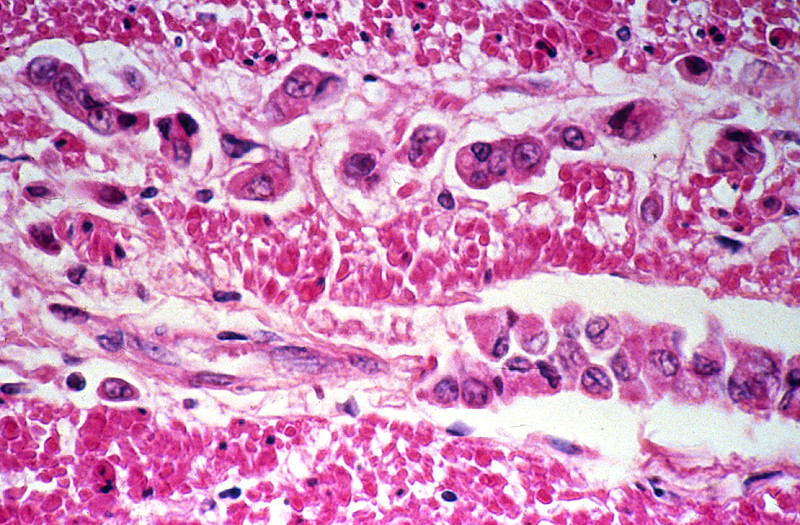
CASE NUMBER 5 Clinical History: This 77-year-old male died from pneumococcal meningitis. The patient had a history of advanced tuberculosis, which had been successfully treated, and mild silicosis. Adenocarcinoma of the prostate with several metastases was an unexpected finding. Gross: The prostate was quite large and firm with multiple rubbery nodules measuring 2 mm to 6 mm in diameter. Some of the nodules contain yellowish flecks. The seminal vesicles were firm bilaterally. Microscopic: There are a number of glands shown in varied patterns. In some cases the epithelial cells are found in non-glandular masses. The epithelial cells are cuboidal or polygonal with central, round, deeply pigmented nuclei. Few, if any, mitotic figures can be seen. The presence of perineural and perivascular invasion is clearly in evidence. This is a useful diagnostic characteristic of adenocarcinoma of the prostate. DIAGNOSIS: Adenocarcinoma of Prostate Image Gallery:
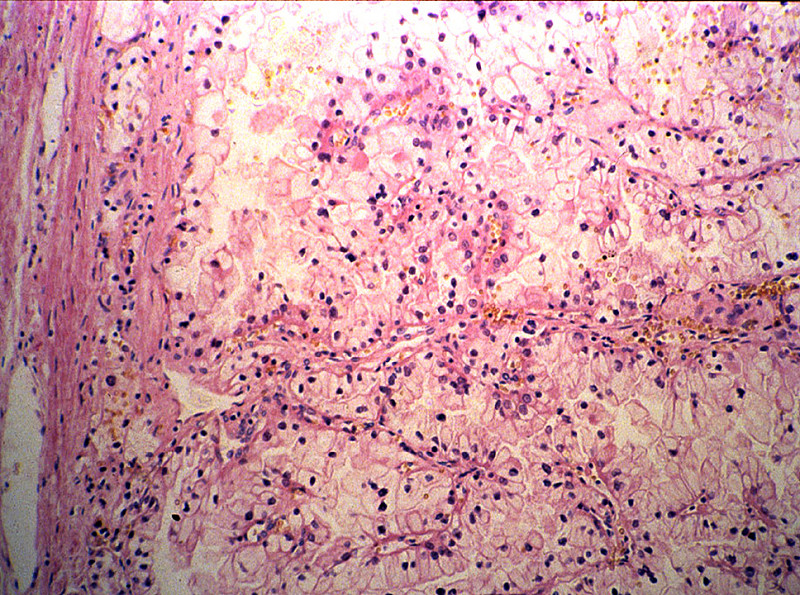
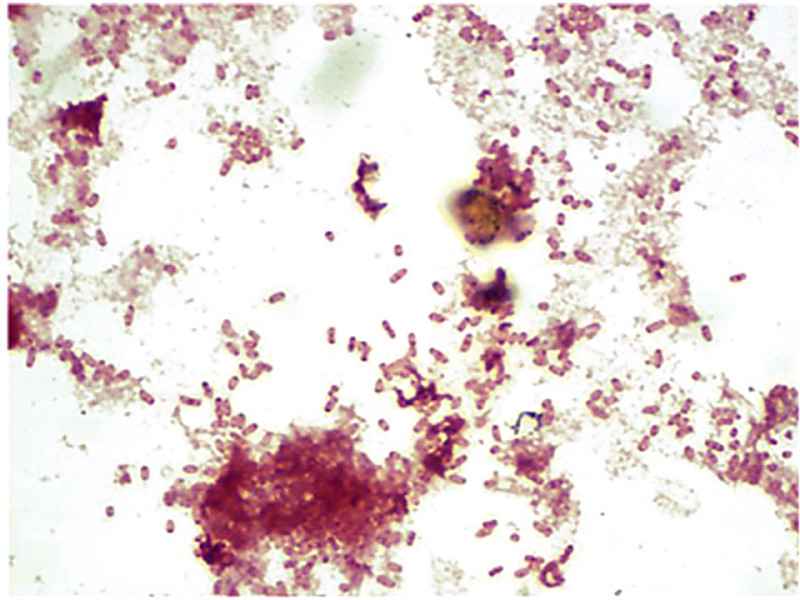
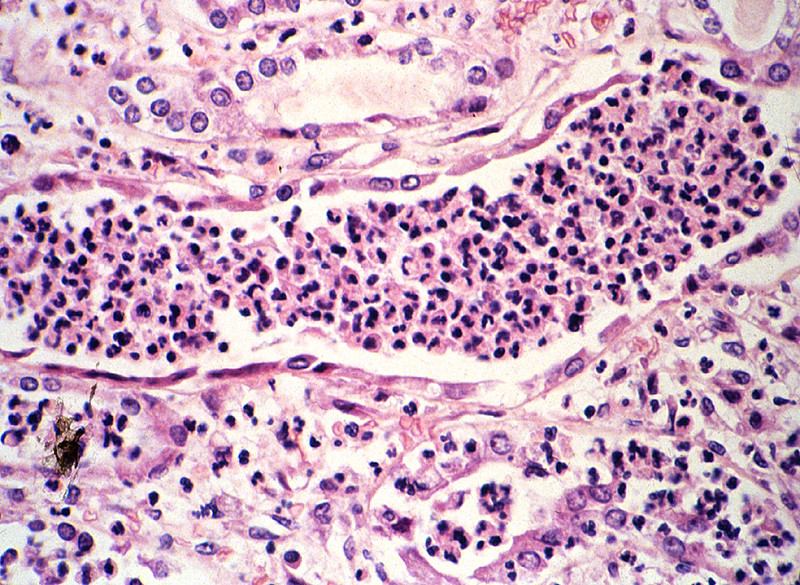
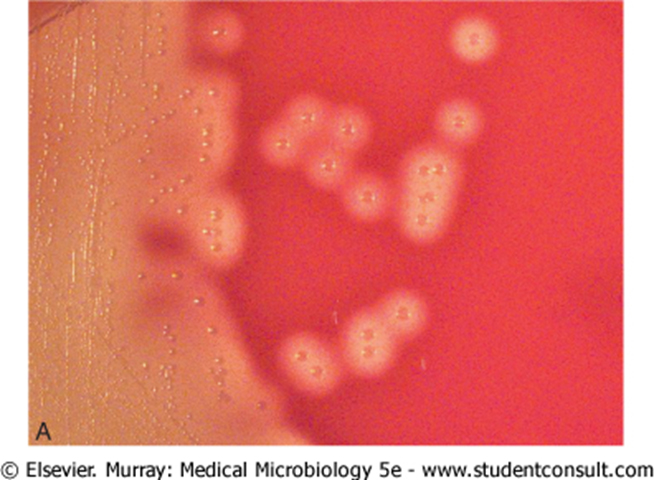
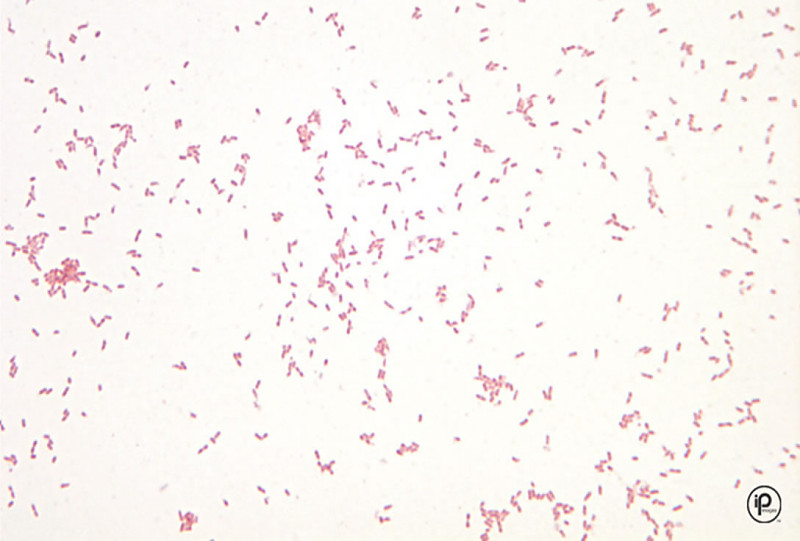
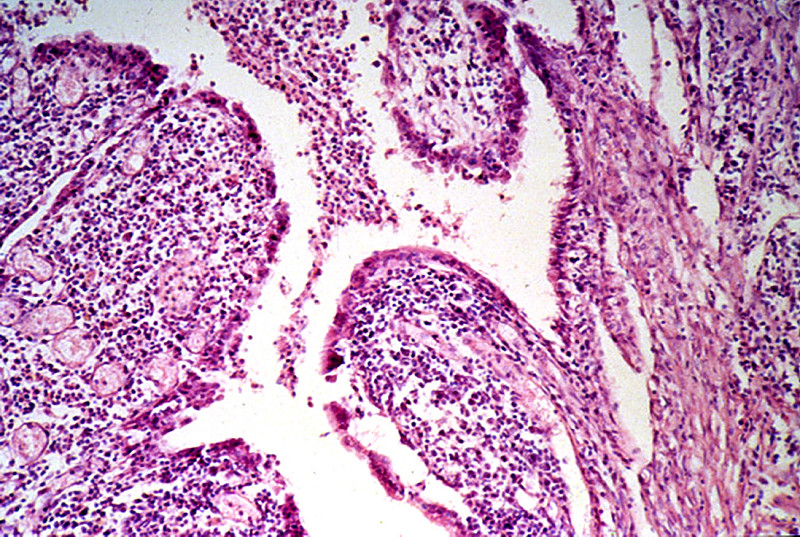
CASE NUMBER 9 Clinical History: A 51-year-old male had a "neurogenic bladder", caused by a spinal cord tumor. He had multiple bladder infections which were treated with antibiotics. He had surgery to remove the tumor. Postoperatively, he developed fever and costovertebral angle tenderness which did not respond to antibiotics. He expired and an autopsy was performed. Gross: The bladder was distended, with a thickened, trabeculated wall. There was a bilateral hydroureter and hydronephrosis. The left kidney was swollen, and the cut surface showed soft foci of yellow streaks extending toward the pelvis. E. Coli was cultured. Lab Findings: A catheterized urine specimen was obtained before death and submitted for culture studies. The organism grew on sheep blood agar (SBA) and on MacConkey agar with over 100,000 colony forming units/ml of urine. Gram stain of a blood culture showed gram negative rods. Microscopic: Naked eye examination of the slide reveals dark streaks extending from the outer cortex to the inner medulla. Microscopically these are foci of acute inflammation, including necrosis and hemorrhage, with masses of polymorphonuclear leukocytes that are also found in many tubules. DIAGNOSIS: Acute Pyelonephritis Image Gallery:
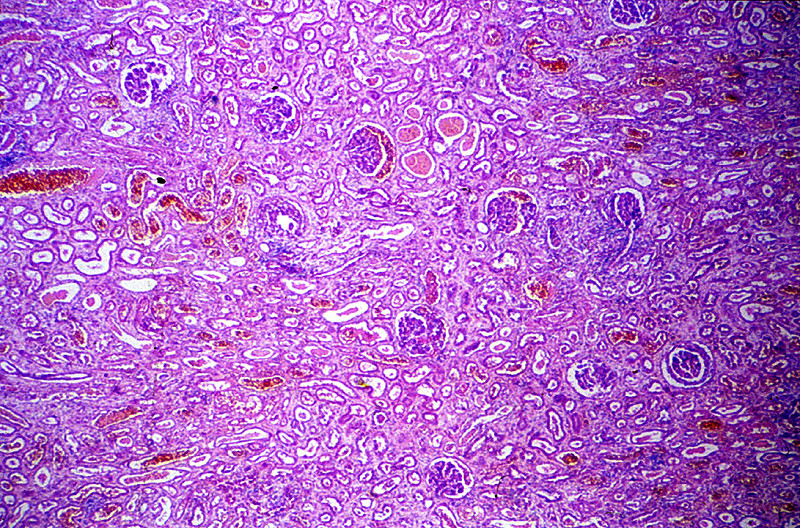
CASE NUMBER 12 Clinical History: A 55-year-old man developed impairment of his vision and was found to have severe hypertension and mild uremia. He was put on a rice diet and improved for several months, but finally died with uremia and pulmonary edema 6 months later. At autopsy, a review of his medical history revealed that he had severe pharyngitis at age 10 requiring bilateral tonsillectomy. Seven days after the tonsillectomy he developed a fever, pain in the region of the costovertebral angles, pyuria, and illness that disappeared after antibiotic treatment. At age 20, he was rejected by the Army because of "proteinuria." Gross: Both kidneys, distorted by multiple irregular broad scars, were small, each weighing about 60 grams. Microscopic: The following features, present in this slide, are characteristic of severe chronic pyelonephritis.Interstitial tissue shows prominent infiltration by lymphocytes and plasma cells, and occasional polymorphonuclear neutrophils; irregular fibrous scars and periglomerular fibrosis. Tubules are dilated, many filled with eosinophilic casts giving the region a "thyroid-like" appearance. A few tubules contain polymorphonuclear neutrophils, indicating that this is an active exacerbation of a chronic pyelonephritis. Arteries are markedly thickened, with intimal proliferation resulting in narrowing of the lumen. Many arterioles show hyaline changes in their walls. Most glomeruli are replaced by fibrous tissue. A few are surprisingly normal in appearance with intact capillaries. There is a prominent peri-glomerular fibrosis in many regions with a thick rim of fibrous tissue circling the outside of Bowman's capsule. DIAGNOSIS: Chronic Pyelonephritis Image Gallery:
CASE NUMBER 14 Gross: The kidneys were both markedly enlarged and pale. Microscopic: The tubular damage here is so severe that it is hard to identify the segment involved. However, it may be noted that most of the necrosis is in the cortex, whereas the collecting tubules in the medulla, although their lumina contain many casts, are lined by relatively intact cells. HgC12 presumably damages mainly proximal convoluted tubules because it is concentrated in this segment. Many involved tubules show marked coagulative necrosis, with sloughing of cells into the lumen. Some tubules that look more nearly normal actually have already have undergone marked necrosis and all that is left is a layer of flattened basilar cells which serve to regenerate the tubule. Regenerative changes can be recognized, including occasional mitoses in epithelial cells. The basement membrane around a few necrotic tubules is broken, and the interstitial tissue contains collections of inflammatory cells and edema fluid. DIAGNOSIS: Acute Tubular Necrosis, Kidney Image Gallery:
CASE NUMBER 17 Clinical History: Four years before death the patient was seen in the hospital because of nausea and vomiting. He had hematuria, proteinuria, urinary casts, and a BUN of 50 mg/dl. A diagnosis of "chronic glomerulonephritis" was made. He did well for over 3 1/2 years, with elevated BUN of 50-60 mg/dl. His blood pressure was 150/90. A month before death his BUN increased and he died of renal failure. Gross: The kidneys were small (80 and 90 grams), and were pale and finely granular. The cortex was markedly thinned. Microscopic: All of the 4 main constituents of the kidney (glomeruli, tubules, vessels, and interstitial tissue) are involved. Although all glomeruli are abnormal, they are not involved to the same degree; some are completely replaced by fibrous tissue, others are only partly scarred, and a few still contain patent capillary loops. The latter have increased mesangial and epithelial cells of Bowman's capsule. The tubules are dilated; some contain red blood cells, but most contain hyaline casts. The interstitial tissue is rather diffusely infiltrated with many lymphocytes and plasma cells. There is a moderate to marked degree of arteriosclerosis. DIAGNOSIS: Proliferative Glomerulonephritis, Severe, Advanced (Chronic) Image Gallery:
CASE NUMBER 18 Clinical History: This 29-year-old male's illness began 10 weeks prior to death, with an episode of "flu". Two weeks later his urine became "smoky". He was found to have hematuria, albuminuria and elevated BUN (180 mg/dl). He died from a pulmonary embolus. Gross: The kidneys were enlarged (230 gm each). The surface was granular and covered with pinpoint hemorrhages in the fresh state. The external surface with capsule removed is illustrated. Microscopic: There is marked proliferation of epithelium of Bowman's capsule producing "crescents". In places fibrin strands are intermixed with the epithelial cells. Tubules are dilated and contain many red blood cells. There is marked interstitial edema and presence of numerous leukocytes. The presence of a large number of crescents is a bad prognostic sign.Image Gallery:
CASE NUMBER 19 Clinical History: This 51-year-old male had tuberculosis for many years. He developed some ankle edema, and was found to have an enlarged liver and 2+ proteinuria. Gross: The heart was large, weighing 470 grams. The liver weighed 1900 grams and was firm with a waxy appearance. Both kidneys were large, each weighing 250 grams. This chronic renal disease may actually increase the size of the kidney. Pale deposits of amyloid are present in the cortex, most prominently at the upper center. Microscopic: Kidney: The same type of hyaline pink material is present in the glomeruli, and is deposited between the endothelial cells and the basement membrane. In some places, it may be present in masses that encroach on the lumen of the capillary. The amyloid can also be recognized in the walls of some small arteries, and in a few places can be seen around the tubules in the interstitial tissue. DIAGNOSIS: Amyloidosis of the Liver and Kidney Image Gallery:
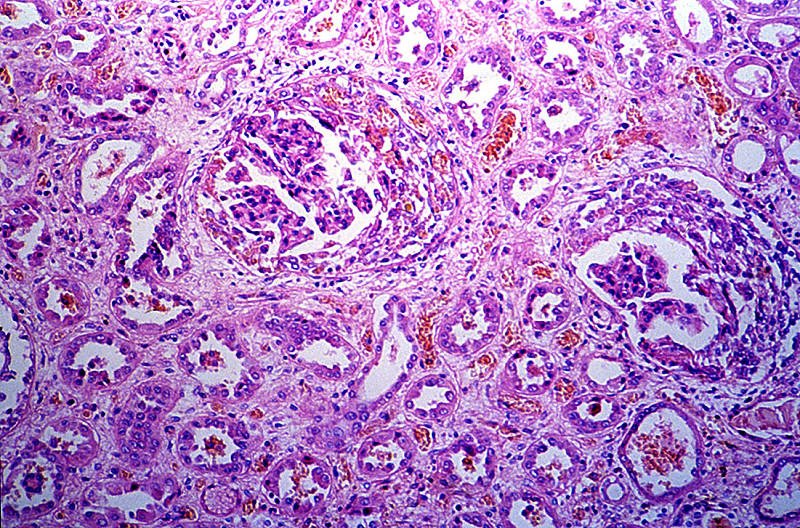
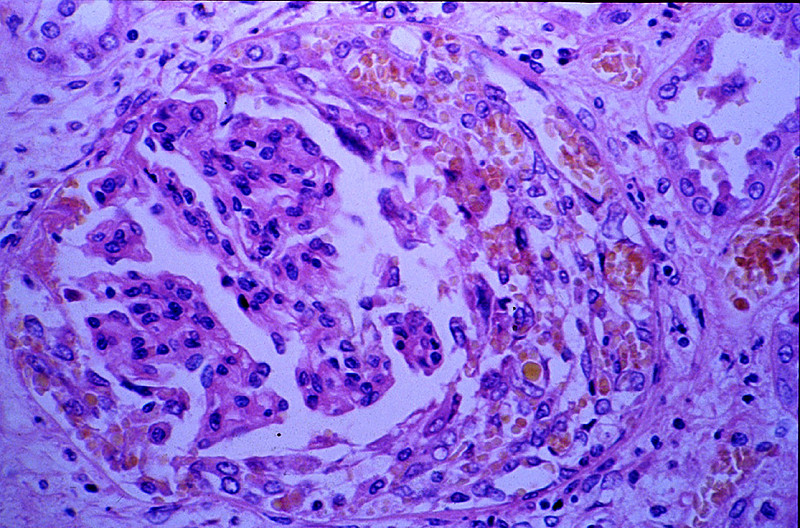
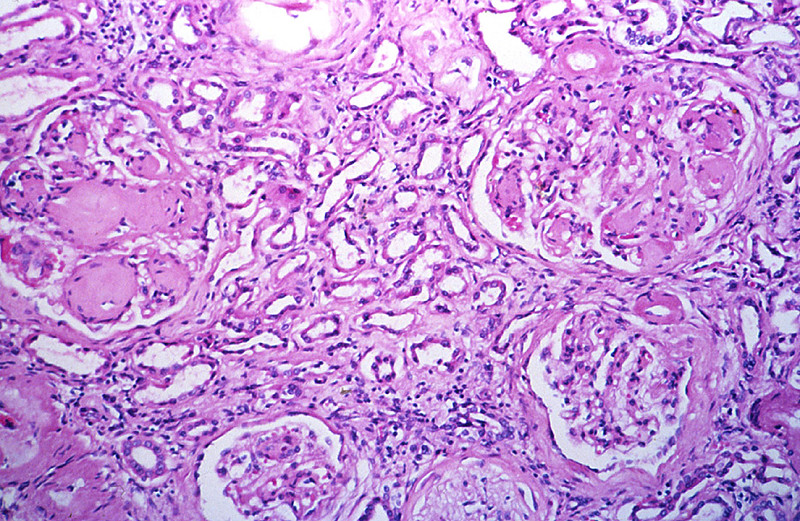
CASE NUMBER 20 Clinical History: This 55-year-old female first came to medical attention when she complained of frequent urination, increased thirst and weight loss at age 15. Insulin dependent diabetes was diagnosed. She developed proteinuria at age 20. Her disease progressed until she became dialysis dependent at age 45. She expired due to pneumonia after a below knee amputation Gross: The kidneys were small and each weighed 100 grams. The surface was irregular with pits and small cysts. Microscopic: There are glomerular lesions consisting of diffuse and nodular glomeroslerosis. Nodular glomerulosclerosis or Kimmelstiel-Wilson lesions are ball-like deposits of PAS positive material which contain trapped mesangial cells. These occur in 15-30% of long time diabetics and are virtually pathognomonic of the disease. Diffuse glomeruloslerosis usually appears as global sclerosis of the glomerular tuft. Chronic pyelonephritis, arterio and arteriolo nephrosclerosis as seen here are also typical findings in diabetic kidneys. DIAGNOSIS: Diabetic nephropathy Image Gallery:
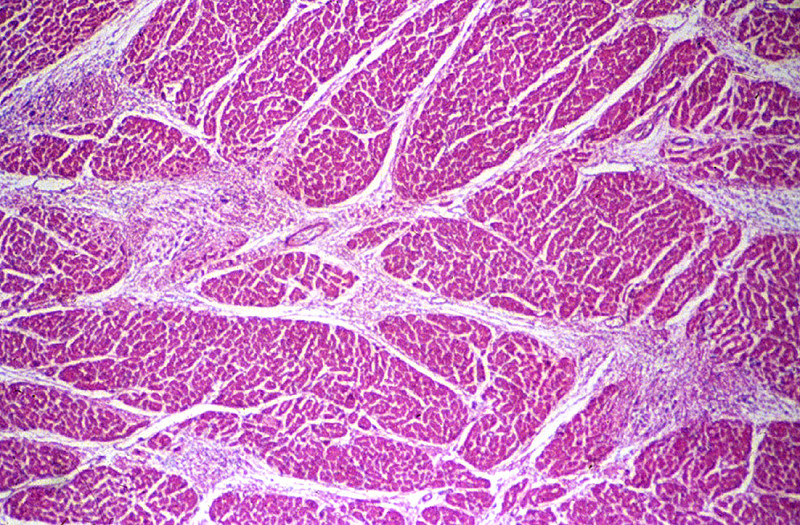
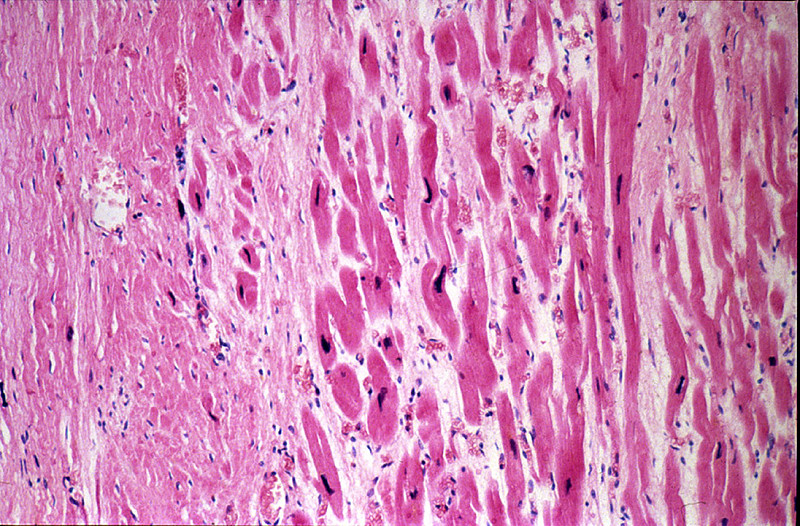
CASE NUMBER 25 Gross: Her heart weighed 380 grams (normal for this age is about 115 grams). The pericardium was covered with a fibrinous exudate. The left ventricle was dilated and the myocardium was flabby. The mitral valve was slightly thickened as were the chordae tendinae. There was a MacCallum's patch in the left atrium. The liver weighed 780 grams (normal 750 grams). There was centrilobular congestion ("nutmeg liver"). Microscopic: The section includes the entire thickness of the myocardium and is taken through the mitral valve so that both left atrial and left ventricular myocardium are present in the section. The epicardium shows a prominent layer of fibrin on the surface; deep to this is young connective tissue with many capillaries, fibroblasts, and chronic inflammatory cells, i.e. granulation tissue. Thus, this is an organizing fibrinous pericarditis. There is also myocarditis present. The myocardial inflammation includes Aschoff bodies of different ages. Identify very early, intermediate and healed foci. The presence of Aschoff bodies indicates that this is a rheumatic myocarditis. Note also marked endocardial thickening due to inflammation and scarring, especially in the left atrium (MacCallum's patch). DIAGNOSIS: Acute Rheumatic Fever of Heart Image Gallery:
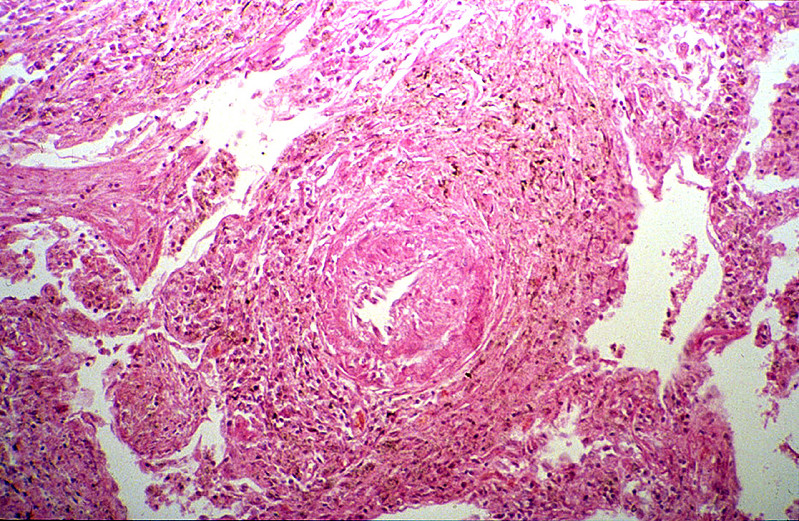
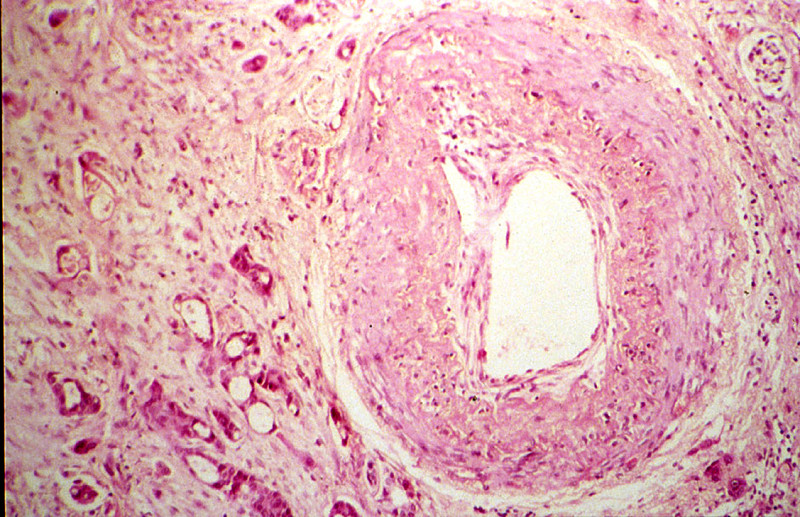
CASE NUMBER 26 Gross: The walls of the gallbladder were thickened. The mucosa of the gallbladder is intact. Yellow tan faceted gallstones are present in this gallbladder. Microscopic: This gallbladder had an unexpected finding. The small arteries in the wall are involved in a necrotizing and inflammatory process which appears to be in all stages of development, resolution, and healing. The earliest change seen is an acute fibrinoid necrosis of the wall of the artery, which appears in the innermost third of the media, frequently involves the wall in an eccentric arrangement, and finally involves the entire thickness of the wall. Many of these arteries are markedly dilated with the formation of aneurysmal-like sacs. There is a marked exudation of inflammatory cells both within the wall of the artery and surrounding the artery. These cells are made up of eosinophils, neutrophils, histiocytes and lymphocytes. In some of the vessels, the process appears to be in a healing phase with the site of artery represented by fibrous scar surrounded by a chronic inflammatory exudate. Arterioles, capillaries, and veins are relatively spared in this necrotizing process. DIAGNOSIS: Polyarteritis Nodosa Image Gallery:
CASE NUMBER 28 Clinical History: A 47 year old female with a history of hypertension of at least 8 months duration noted sudden onset of severe inter-scapular pain which rapidly radiated to base of neck but not to abdomen 7 hours prior to admission. On admission her BP was 160/130 (both arms) and pulse was 80 and equal bilaterally. No murmurs were noted. A retrograde aortogram revealed a double channel extending from the root of the aorta to the innominate artery. Aortotomy was performed for attempted repair of the dissecting aneurysm, but during the procedure there occurred an adventitial tear with subsequent hemopericardium and cardiac tamponade. The patient expired on the operating table 6 hours after surgery had begun. Gross: The heart weight was 550 grams and there was left ventricular hypertrophy. The aorta had an intimal tear at the base of the innominate artery with dissection of the media occurring in the outer 2/3 and extending proximally to within 0.5 cm of the aortic valve. There was an adventitial tear at this point. Microscopic: There is a blood-filled tear between the inner 2/3 and outer 1/3 of the media. Note necrosis and deposition of fibrin along the margins of the defect. The remainder of the media contains the changes of "cystic medial necrosis" DIAGNOSIS: Dissecting Aneurysm, Ascending Aorta, with cystic medial necrosis Image Gallery:
CASE NUMBER 30 Clinical History: This 80-year-old woman had been known to be hypertensive for many years. She died of congestive heart failure, following a period of hospitalization for pneumonia. Gross: The heart was enlarged. Both kidneys were somewhat smaller than normal (100 grams each) and were finely and diffusely granular. Microscopic: The arterioles are prominent with hyalinized walls. Note the thickened arterioles at the vascular poles of the glomeruli, and observe the extension of the hyaline material into the glomerulus. Some glomeruli are more scarred than others. This "sclerosis" is secondary to the ischemia caused by the narrowed lumens of the arterioles. There are also scattered patches of interstitial fibrosis and chronic inflammation. DIAGNOSIS: Arteriolar Nephrosclerosis Image Gallery:
CASE NUMBER 31 Clinical History: This 45-year-old man had been well until he was awakened by chest pain that radiated to both arms and neck and was associated with diaphoresis. His blood pressure was 160/110. He was treated with diuretics (Lasix), but despite this he continued to gain weight. Two days after the onset of the chest pain he had a cardiac arrest which was preceded by third degree heart block. Gross: The heart was slightly enlarged weighing 460gms. There was severe atherosclerosis of all the major coronary arteries with a recent thrombotic occlusion of the proximal right coronary artery. A recent transmural infarct was present in the left ventricle that involved the posterior interventricular septum and the posterior papillary muscle. Microscopic: The slide includes a transmural section of the posterior wall of the left ventricle. Nearly the entire section is involved by infarct. However, there is a thin rim (5 to 10 cell layers) of endocardial myocytes which have survived because of diffusion of oxygen and nutrients from the ventricular cavity. Other viable myocytes can be found around larger blood vessels within the section. The intense hypereosinophilia of the necrotic myocytes can best be appreciated by comparing the thin rim of lighter staining subendocardial myocytes with the deeper cells. Note also the karyolysis that is characteristic of coagulation necrosis. In some areas there is little inflammatory response. This observation is explained by microvascular necrosis which does not allow access of circulating leukocytes to these areas. In other areas, especially in the epicardial half of the infarct, there is an intense acute inflammatory response. Many intact neutrophils can be seen. In addition, there are many nuclear fragments from lysed neutrophils. Macrophage activity is not evident. These features of the inflammatory response indicate that the infarct was approximately three to four days old. Note also that the inflammation extends to the epicardial surface and that there are deposits of fibrin on the epicardium. This is called fibrinous pericarditis. The granular grey material seen within some blood vessels is barium sulfate, which was injected to permit post-mortem study of the coronaries by radiography. DIAGNOSIS: Recent Myocardial Infarct Image Gallery:
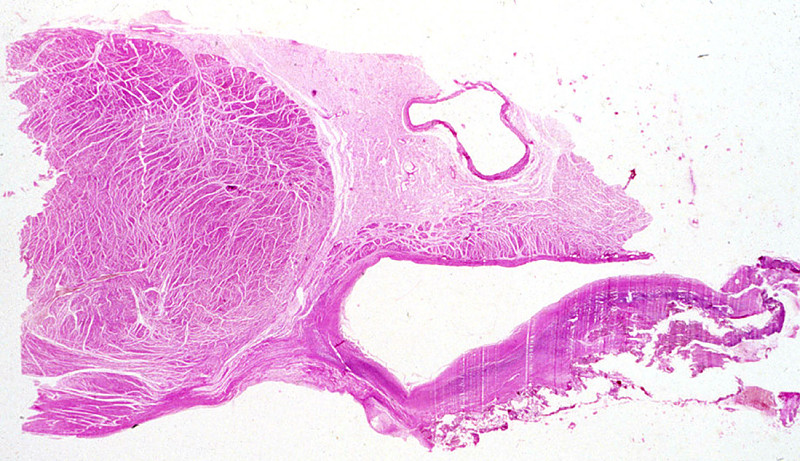
CASE NUMBER 33 Clinical History: This 57-year-old female complained of hematuria. She was cystoscoped and found to have a papillary mass near the dome of the bladder. Microscopic: Orient yourself by naked-eye and low power examination in regard to the 3 main layers of the bladder wall. A normal transitional epithelium lines about 1/2 of the mucosal surface. The central portion is thrown up into many fingerlike fronds (papillae). The connective tissue and vascular core is line by thickened, atypical transitional epithelium. There is a suggestion of very early invasion into the mucosa at the base of the tumor but the muscularis is uninvolved. DIAGNOSIS: Papillary Transitional Cell Carcinoma of Urinary Bladder Image Gallery:
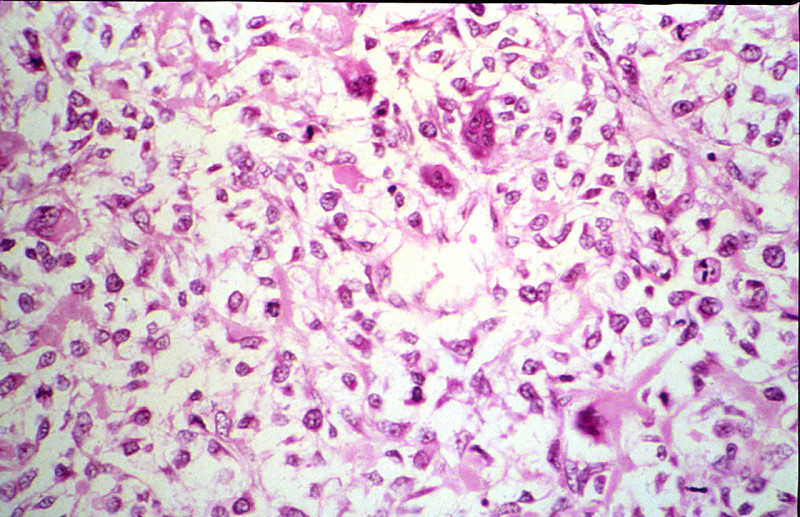
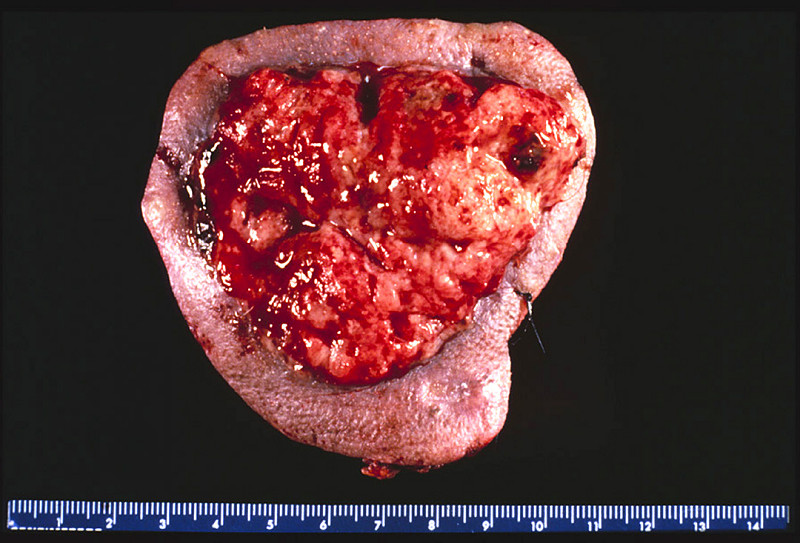
CASE NUMBER 34 Clinical History: This 48-year-old white male had a history of embryonal carcinoma and seminoma of the left testis when he was 37. A mass was noted on the remaining right testis. An orchiectomy was done. Gross: The orchiectomy specimen has been opened to demonstate the soft fleshy tumor which has replaced the normal testis. The spermatic cord is attached. Microscopic: Note the characteristic arrangement of cells in small groups outlined by delicate fibrous stroma. The cells are relatively uniform with distinct borders. The cytoplasm is clear and sometimes almost foamy. The cells are polygonal with large, round, central nuclei and prominent nucleoli. In many sections a fragment of atrophic and fibrotic testis may be seen adjacent to the tumor. DIAGNOSIS: Testicular Seminoma Image Gallery:
CASE NUMBER 35 Gross: Recent infarcts are seen in Kidneys, Brain, Spleen Microscopic - Kidney: There is recent infarct in this section, with a central area containing "ghosts" of tubules outlined by a marginal zone of polymorphonuclear neutrophils, necrotic debris, and hemorrhage. Some tubules immediately beneath the renal capsule are spared. An artery in the medulla contains a thrombo-embolus that presumably originated from the thrombus on the mitral valve. DIAGNOSIS: Recent Infarct, Kidney Image Gallery:
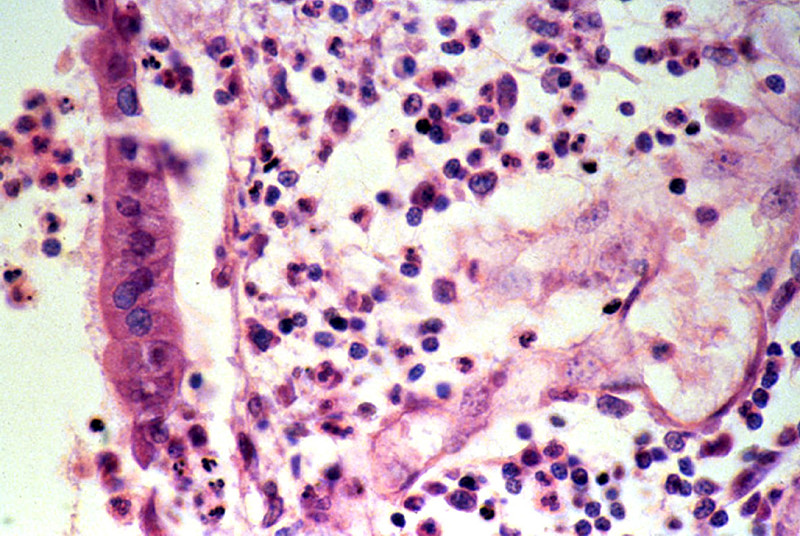
CASE NUMBER 39 Clinical History: A 58-year-old African American female had been hemiplegic on the right for a period of 3 months prior to death. She developed fever and dyspnea several days prior to death. Gross: There was a thrombosis of the left internal carotid artery with infarction of the left cerebral hemisphere. There was a massive embolus of the right pulmonary artery. Both lungs were firm with mucopurulent exudate in and about the bronchi. The left lower lobe was firm and gray-yellow with a shaggy fibrinous exudate over the pleura. (E. Coli and Proteus mirabilis were cultured from this area). Microscopic: Bronchi and alveoli are filled with neutrophils. There are scattered masses of fibrin. DIAGNOSIS: BronchopneumoniaImage Gallery:
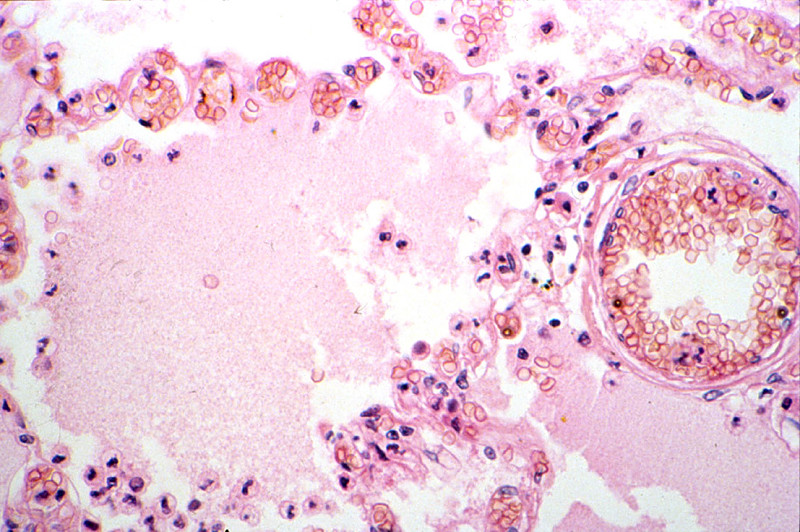
CASE NUMBER 40 Clinical History: A 45-year-old male entered the hospital two days prior to death for evaluation of seizures during the previous month. The neurologic examination was unremarkable. The only symptoms consisted of two seizures. He was found dead by the nurse. Gross: Both lungs were heavy, wet, slightly firm, and dark-red. Microscopic: The alveoli are filled with a homogeneous pink material. The septal capillaries are engorged with blood. An incidental finding consists of anthracotic pigment near the pleural space DIAGNOSIS: Pulmonary Edema Image Gallery:
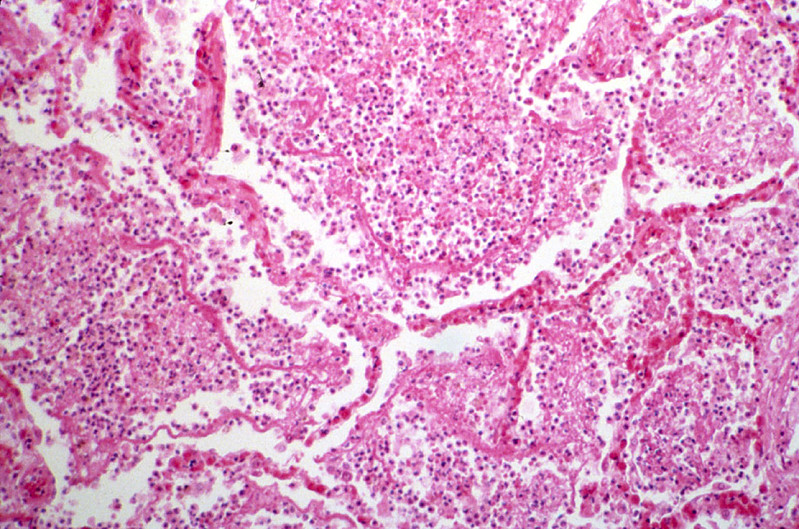
CASE NUMBER 46 Gross: Both lungs were heavy, firm, and dark red. There were numerous firm gray areas up to 0.3 cm. in all lobes. Microscopic: The alveoli were filled with eosinophilic material representing fibrin. There is early proliferation of fibroblasts in some of these areas. At the periphery there are neutrophils and mononuclear cells. Note the marked alveolar hemorrhage. Brown, granular pigment is present in scattered macrophages. This is hemosiderin. Alveolar hemorrhage may be related to the acute glomerulonephritis that was also present in this patient. Note the diffuse neutrophilic infiltrate in alveolar walls. DIAGNOSIS: Organizing Bronchopneumonia Image Gallery:
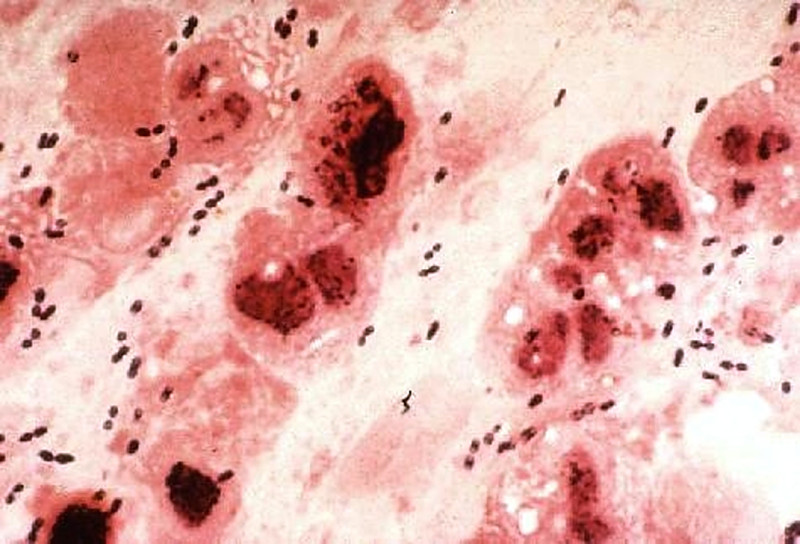
CASE NUMBER 51 Clinical History: A 45-year-old male became ill approximately 2 to 3 weeks ago following an alcoholic spree. He had nausea, vomiting, dehydration, confusion and high fever. He died suddenly shortly after admission. Lab Findings: Gram stain of sputum obtained before death shows Gram positive cocci in pairs. Gross: The right lung was heavy weighing 700 grams. Its lower lobe showed diffuse gray consolidation. The trachea and bronchi contained a great deal of mucus, and the mucosa was dark red. Microscopic: The alveoli are distended and contain a large amount of inflammatory exudate, which consists of many polymorphonuclear leukocytes, a few RBC's, macrophages and strands of fibrin. Many RBC's have been phagocytosed by the macrophages and are undergoing disintegration. The alveolar septa are delicate and well preserved, but markedly congested. DIAGNOSIS: Lobar Pneumonia, Gray Hepatization Stage Image Gallery:
CASE NUMBER 54 Clinical History: An 18-year-old female had nausea, vomiting, periumbilical and lower abdominal pain, shaking chills and fever beginning two days ago. The WBC count was 21,900. Physical examination revealed local tenderness and rigidity with rebound pain in the lower abdomen. Gross: The appendix was swollen, dark red, hemorrhagic, and covered by gray-yellow exudate. Serial cross-sections revealed a distended lumen containing hemorrhagic material and a fecalith, which apparently obstructed the lumen. Microscopic: Portions of the mucosa are ulcerated, necrotic and heavily infiltrated with neutrophils. This acute inflammation and necrosis extends throughout the entire thickness of the wall and the serosa. In the appendicial lumen there is pus and a fecalith. DIAGNOSIS: Acute Suppurative Appendicitis with Perforation Image Gallery:
CASE NUMBER 70 Clinical history: This 60-year-female presented to her physician with a complaint of post menopausal bleeding. Gross: The surgical specimen was an enlarged uterus, distorted by multiple firm, grayish-white nodes and nodules (myomata). Within the endometrial cavity was a pedunculated grayish-red mass with smooth surfaces, measuring about 2.5 x 1 cm, lying in the long axis of the uterus. Microscopic: A pedunculated, endometrial polyp arises from the endometrial surface. It is composed of distorted endometrial glands of various sizes, some of which show cystic dilatation. The glands are lined by one or more rows of cells with uniform oval or round nuclei and scanty, eosinophilic cytoplasm. The lumina contain a small amount of mucoid secretions. The surrounding stroma shows slight diffuse, lymphocytic infiltration. The endometrium adjacent to the polyp shows pressure atrophy and focal hemorrhages. Located submucosally and within the myometrium are two small leiomyomas. DIAGNOSIS: Uterine endometrial polyp Image Gallery:
CASE NUMBER 79 Clinical History: A 45-year-old male entered the hospital two days prior to death for evaluation of seizures during the previous month. The neurologic examination was unremarkable. The only symptoms consisted of two seizures. He was found dead by the nurse. Gross: The combined weight of the adrenals was 19 grams. There were several yellow cortical nodules up to 0.6 cm in diameter. Microscopic: Observe without the microscope the nodule of tissue at one end of the section. The cells are mostly in a fascicular arrangement. They are vacuolated and histologically appear identical to normal cortical cells. DIAGNOSIS: Cortical Adenoma, Adrenal Image Gallery:
CASE NUMBER 81 Clinical History: This 62-year-old white male had a history of alcoholism. Two months prior to death he vomited blood. One month before death there was a massive gastrointestinal hemorrhage. He expired following an attempt to ligate esophageal varices. Gross: The liver weighed 1800 grams. The entire organ was uniformly composed of nodules about 0.5 cm in diameter, each surrounded by fibrous tissue. The organ was jaundiced and firm. Microscopic: The usual architecture present in the liver has been completely disrupted by the bands of connective tissue. In these bands one sees chronic inflammatory cells, mainly lymphocytes and other mononuclear cells. There is some proliferation of the bile ductules. DIAGNOSIS: Micronodular Cirrhosis Image Gallery:
CASE NUMBER 84 Clinical History: This 84-year-old female developed weakness and weight loss six months prior to death. She saw a physician twelve days prior to death with signs and symptoms of intestinal obstruction. A tumor mass was palpated in the rectum. She returned home and died with intestinal perforation. She was unable to eat during the last several days of life. Gross: The peritoneal cavity contained fecal material. A 1 cm perforation was present in the sigmoid colon. The bowel was markedly distended and filled with fecal material. There were numerous large superficial ulcerations of the large bowel. A tumor was present 4 cm from the anus. It was hard and had completely surrounded the bowel, reducing the lumen to less than 0.5 cm in diameter. Small tumor implants were present over the peritoneum and mesentary nearby. No distant metastases were noted. Microscopic: Inspect the slide first without the microscope. The remainder of the lumen of the bowel can be recognized. Note the thickened bowel wall and masses of tumor surrounding fat. Under low power note the tendency in some areas toward a gland-like structure. There is considerable variation in nuclear staining, size and shape. In some areas clumps of tumor cells are in the midst of mucus which the tumor cells are producing. Note the relatively large amount of dense collagen which accompanies the tumor cells in the fat. DIAGNOSIS: Adenocarcinoma of Rectum Image Gallery:
CASE NUMBER 85 Clinical History: This 84-year-old white female developed weakness and weight loss six months prior to death. She saw a physician twelve days prior to death with signs and symptoms of intestinal obstruction. A tumor mass was palpated in the rectum. She returned home and died with intestinal perforation. She was unable to eat during the last several days of life. Gross: The liver weighed 980 grams. The lobular pattern was accentuated with central areas appearing red and other areas yellow. Microscopic: The areas of fatty change are readily visible with use of scanning power. They are zonal. Note the peri-portal areas are severely involved and the areas of fatty change extend from one portal area to another. The more severely involved cells have eccentric nuclei and the entire cytoplasm is replaced by a fat globule. DIAGNOSIS: Fatty Liver Image Gallery:
CASE NUMBER 89 Clinical History: This 73-year-old female presented with right upper quadrant pain and elevated WBC count. Physical exam revealed right upper quadrant tenderness. Ultrasound examination of the gallbladder revealed gallstones. Gross: The gallbladder was thickened and hyperemic. No localized masses were seen. The gallbladder contained numerous gallstones. Microscopic: The gallbladder mucosa is acutely inflamed with many neutrophils in the epithelium and lamina propria. The epithelium is reactive with enlarged nuclei and abundant eosinophilic cytoplasm and ulcerated in some areas. There is hemorrhage and fibroblastic proliferation throughout the wall. Chronic cholecystitis is evidenced by plasma cells in the mucosa and Rokitansky-Aschoff sinuses which are diverticular invaginations of mucosa in the gallbladder wall. No tumor is seen. DIAGNOSIS: Acute and Chronic Cholecystitis Image Gallery:
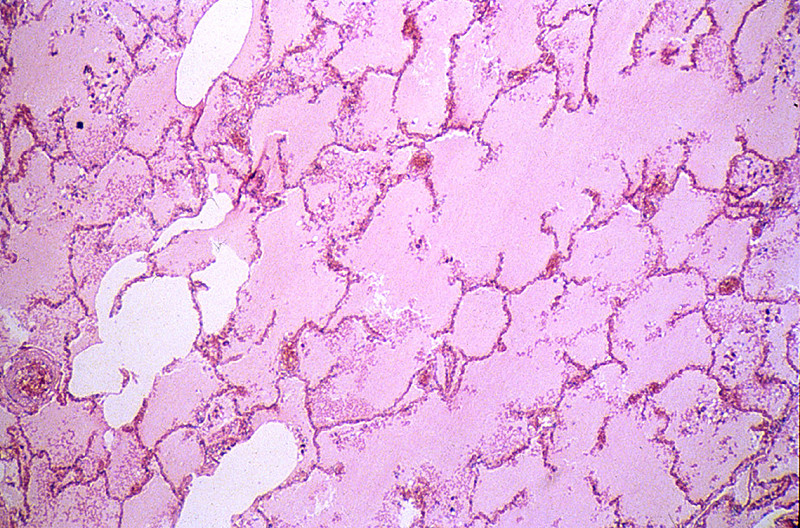
CASE NUMBER 92 Clinical History: A 65-year-old male complained about increasing dyspnea over the last 10 years. The dyspnea had suddenly increased and the patient was admitted with signs of heart failure. He died one week after admission from an acute brain infarct. Gross: The lungs were very large and even though he had lived in a large metropolitan area all his life, his lungs were light gray in color. The medial edges of the lungs met the midline. Upon palpation there was marked crepitation. Microscopic: The alveolar spaces are distended and the alveolar septa are thickened by fibrous tissue. Numerous "free floating" alveolar septa are present, recognizable as pieces at alveolar wall not connected at either end to adjacent septa. DIAGNOSIS: Centrilobular Emphysema Image Gallery:
CASE NUMBER 93 Clinical History: A 30-year-old female had recurrent bouts of severe abdominal pain accompanied by elevated serum amylase. Partial pancreatectomy was performed for relief of chronic pain, unresponsive to medical therapy. Gross: Fibrosis obscured some areas of pancreas architecture. Saponification of peripancreatic fat was seen in small foci. Microscopic: Several areas of fat necrosis with adjacent neutrophil infiltrate are seen, evidence of acute pancreatitis. In addition, some lobules of the pancreas show fibrosis and loss acini, evidence of chronic pancreatitis. In these areas, islets of Langerhans appear larger and more abundant. This is partly because they are resistant to injury and persist when acini are destroyed and partly because they undergo reactive hyperplasia DIAGNOSIS: Acute and Chronic Pancreatitis Image Gallery:
CASE NUMBER 95 Clinical History: A 60-year-old white male had a resection of the right side of colon for adenocarcinoma. Seven days after the operation he had continuous abdominal discomfort and went into shock. A laparotomy revealed that the entire small bowel was gangrenous. Gross: The jejunum and ileum were dark red, thickened and indurated. The mucosal surface was covered by bloody mucus. The cut surface revealed hemorrhages throughout all layers of the intestinal wall. The superior mesenteric vein and its tributaries were obstructed by dark red thrombi which were attached to the vascular wall. Microscopic: The villi are swollen. The superficial layer of the mucosa is necrotic and contains clumps of bacteria. The deeper layer of the mucosa is hemorrhagic but epithelial cells are relatively well preserved. A severe degree of edema, congestion and hemorrhage is seen throughout the submucosa and muscularis layers. The muscle cells are not yet necrotic. DIAGNOSIS: Hemorrhagic Infarct, Ileum Image Gallery:
CASE NUMBER 98 Clinical History: This 70-year-old man worked in a rock quarry as a crusher for 18 years. Six months prior to death he began to have dyspnea, orthopnea, paroxysmal nocturnal dyspnea and ankle edema. He was admitted for congestive heart failure and died suddenly with massive pulmonary embolism. Gross: Both lungs were heavy, 900 grams for the left lung and 1120 grams for the right one. The lung was slate gray and firm. Microscopic: In the left upper part of the section the characteristic lesions of silicosis are seen. There are masses of fibrous tissue which form concentric lamination around the blood vessels, and stellate scars when the fibrosis extends to the adjacent alveolar septa. A large amount of coal-black pigment and small crystals are found in the macrophages and the scar tissue. These crystals are best seen under polarized light. In advanced lesion the fibrous nodules become confluent as seen in the lower right part of this section. Notice the presence of arteriosclerosis and organizing thrombi in the pulmonary arteries and chronic inflammation of bronchi. DIAGNOSIS: Silicosis of the Lung Image Gallery:
CASE NUMBER 111 Clinical History: This 51-year-old white female had bloody diarrhea which responded to immunosupressant therapy for many years. Her symptoms progressed and portion of the colon was removed. Gross: The mucosa showed an area of edema and hyperemia distally. This was sharply demarcated from the remainder of the colon. A superficial mucosal lesion was noted. Microscopic: This section shows fulminant ulcerative colitis with areas of ulceration extending into the submucosa and also some areas of hemorrhage. While deep ulceration is seen, there is no fissuring necrosis, fibrous expansion of the submucosa, or transmural chronic inflammation, which differentiates this lesion from Crohn's disease. The base of the ulcerated area is covered by necrotic debris and fibrinopurulent or sanguinous exudate. Glands are distorted in shape, infiltrated by neutrophils, and lined by regenerating epithelium. DIAGNOSIS: Ulcerative Colitis Image Gallery:
CASE NUMBER 116 Clinical History: This 50 year female complained of lower abdominal pressure. A mass was palpated on pelvic examination. Gross: A hysterectomy and salpingoophorectomy was performed. The uterus is grossly normal. One ovary is markedly enlarged and replaced by multiloculated cysts. When the cysts are opened they are found to be filled with thick mucinous material. Microscopic: The cysts are complex and lined by benign mucin secreting epithelium. DIAGNOSIS: Pseudomucinous ovarian cystadenoma Image Gallery:
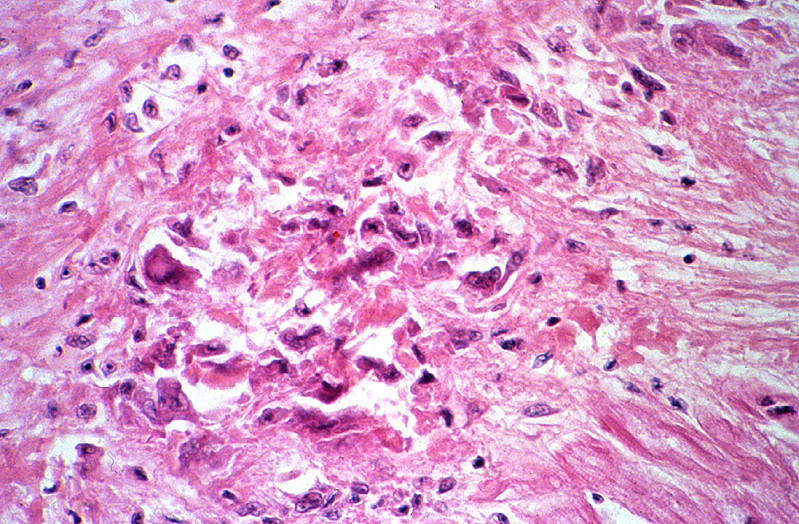
CASE NUMBER 121 Clinical History: A 59-year-old white female had rheumatoid arthritis over a number of years. Subcutaneous nodules were present over the extensor surfaces of the arms. One of these was surgically excised. Gross: A photograph of the patient's elbow is shown. Sometimes persons with rheumatoid arthritis (RA) have rheumatoid nodules form in subcutaneous locations at pressure points, such as the elbow shown here. Rheumatoid nodules may also appear viscerally, such as on the pleura of the lung. Microscopic: There are cellular areas with a stellate shape representing necrosis of collagen. At the periphery is a zone of cells with nuclei oriented perpendicular to the area of necrosis. These are histiocytes. The outer zone contains chronic inflammatory cells and fibrous tissue. DIAGNOSIS: Rheumatoid Nodule Image Gallery:
CASE NUMBER 123 Clinical History: A 45-year-old female presented with a five-month history of irregular and prolonged menstrual periods and pelvic pain. The clinical diagnosis was fibroid uterus. Gross: The tubes were markedly distended and thickened with adhesions between the fimbriated end and the ovaries. On sectioning, pus exuded from the lumen. Microscopic: The villi are plump and edematous, with marked dilation and congestion of capillaries. The mucosa is heavily infiltrated by polymorphonuclear leukocytes, which have broken through foci of necrotic mucosa, producing the purulent exudate. Besides this acute phase, there are chronic features evidenced by plasma cell, lymphocytic and macrophage infiltration and fibroblastic proliferation. The muscular layers are edematous and infiltrated by acute and chronic inflammatory cells. This probably represents gonorrheal infection, the mucosa being predominantly involved, in contrast to other pyogenic infections which more frequently involve the outer layers and relatively spare the mucosa. DIAGNOSIS: Acute and Chronic Salpingitis Image Gallery:
CASE NUMBER 126 Clinical History: This 50-year-old male had respiratory difficulties for some time which increased in severity. Upon admission a large mass was seen in the X-ray films of the lung. The patient suddenly collapsed into a coma and died the following day from massive hemorrhage into a large brain metastasis. Gross: The lungs were remarkable for a 5 cm mass in the right upper lobe. The cut surfaces were friable and yellowish-gray. Regional lymph nodes were filled with similar necrotic tumor. Microscopic: The tumor tissue consists of glandular structures with very large nuclei which are often arranged in several layers. The nuclear to cytoplasmic ratio is low. There are several mitoses and the stroma contains increased amounts of collagen. Well differentiated adenocarcinomas, with a glandular pattern like this one, are uncommon in the lung. DIAGNOSIS: Adenocarcinoma of the Lung Image Gallery:
CASE NUMBER 129 Clinical History: A 70-year-old white male had an insidious onset of dysphagia of six months duration. X-ray revealed a filling defect and stenosis in the lower esophagus. An esophageal resection was performed. Gross: The resected esophagus contained a firm, raised, pink-gray, friable and necrotic 3.5 x 4.5 cm tumor mass, completely encircling the esophagus and producing a marked stenosis. Microscopic: At one end of the section the squamous epithelium of the esophagus shows marked atypia, pleomorphism and loss of polarity, but no submucosal invasion. These changes represent carcinoma in situ. By following the mucosal lining, one comes upon an area where the cords and nests of poorly differentiated squamous cells are seen to invade the mucosa and submucosa reaching the muscular layer. At one margin of the section the tumor cells are better differentiated with production of keratin and formation of so-called epithelial pearls. Associated with the tumor are marked fibrous proliferation and intense chronic inflammatory infiltration in the stroma. The tumor invades into, but not through the muscularis externa. DIAGNOSIS: Squamous cell carcinoma of the esophagus Image Gallery:
CASE NUMBER 133 Clinical History: This 39-year-old male had a history of non-healing rectal fistula and a long standing history of enteritis. There was bloody and mucous diarrhea. Part of the colon was resected due to bowel obstruction. Gross: The colon showed extensive ulcerations separated by pedunculated areas of hypertrophic mucosa. The intestinal wall was swollen and edematous. The serosa was thickened with fibrous adhesions. Microscopic: A broad area of ulceration extends into the submucosa. The surface of the ulcer is covered by fibrinopurulent exudate overlying granulation tissue. Neutrophils infiltrate glands in the adjacent mucosa, some of which are lined by regenerating epithelium. A few crypts are distorted in shape. These features differ little from those seen in ulcerative colitis (Case No. 111). However, this section also shows transmural chronic inflammation in the form of lymphoid aggregates and granulomatous inflammation. DIAGNOSIS: Granulomatous Colitis (Crohn’s disease) Image Gallery:
CASE NUMBER 134 Clinical History: An 81-year-old, asymptomatic female was found to have guaiac positive stool on routine examination. Flexible sigmoidoscopy revealed a rectal mass. Gross: A 5 cm fungating, centrally ulcerated mass was found on gross examination. Microscopic: This section, which includes the edge of the tumor shows invasive adenocarcinoma arising in a villous adenoma. Tall villi lined by neoplastic epithelium replace the normal mucosa at the edge of the mass. Centrally, where the lesion was ulcerated, tumor infiltrates through the muscularis propria and in some sections, enters the subserosal adipose tissue. Irregular glandular spaces are lined by tumor cells and large pools of mucin are seen, as well as desmoplastic (fibrotic) stroma. Although the nuclei of the carcinoma are anaplastic when compared to the normal colon mucosa, the neoplastic epithelium retains a columnar appearance, typically seen in colon carcinoma. DIAGNOSIS: Adenocarcinoma of Colon
CASE NUMBER 135 Clinical History: A 57-year-old female had satiety, deep epigastric pain, nausea and vomiting for two months. An upper GI series revealed a small ulcer in the stomach. The free gastric acidity was low, and there was occult blood in the stool. A total gastrectomy was performed after the diagnosis of malignancy was made from a frozen section. Gross: A shallow ulcer 1 cm in diameter was in the anterior wall of the stomach, 7 cm proximal to the pylorus. There was a broad zone of induration and thickening of the gastric mucosa which surrounded the ulcer. The section showed a diffuse gray-white mucosa tightly adherent to its submucosa. The submucosa is considerably thickened. Microscopic: The ulcer is covered by a thin layer of inflammatory exudate. Granulation tissue and lymphocytic infiltration are present at the ulcer base. There is extensive fibrosis throughout the entire wall of the stomach with scattered tumor cells arranged in small clusters and in chains. These tumors cells are often hard to distinguish from the inflammatory cells. DIAGNOSIS: Adenocarcinoma, Stomach (Linitis Plastica) Image Gallery:
CASE NUMBER 139 Clinical History: A 68-year-old man was found to have guaiac positive stools. Colonoscopy revealed a sigmoid colon mass. Elevated liver function tests raised the suspicion of metastases and CT scan showed a liver mass. The colon primary was resected and a partial hepatectomy was performed. Gross: An 8 cm area of liver was replaced by a tumor mass. The tumor was firm and white in comparison to the surrounding soft, golden brown liver. Areas of hemorrhage and necrosis could be seen within the tumor. Microscopic: A small portion of residual liver can be seen in most sections. The tumor mass is made up of irregular glandular spaces lined by malignant, cuboidal to columnar epithelium. The neoplastic glands are dispersed in desmoplastic (fibrotic) stroma. DIAGNOSIS: Metastatic Colon Carcinoma in Liver Image Gallery:
CASE NUMBER 143 Clinical History: This 21-year-old woman had an implant of plastic (etheron) material in her left breast. This was done for cosmetic purposes. The implant caused severe inflammation and had to be removed. Microscopic: The irregular fragments of foreign material are surrounded or engulfed by multinucleated foreign body giant cells. The rest of the section is made up of fibrous connective tissue and collections of lymphocytes and histiocytes. DIAGNOSIS: Foreign Body Reaction Image Gallery:
CASE NUMBER 154 Clinical History: A 64-year-old man complained of hoarseness and throat pain. Gross: A tumor involved the right true and false vocal cord and extended across the midline. Microscopic: The mucosa is partially columnar, representing the ventricular mucosa. There is a transition to squamous mucosa with marked nuclear pleomorphism. The abnormal squamous cells extend into the underlying stroma where the cells keratinize. Focal necrosis and an inflammatory infiltrate is present. DIAGNOSIS Squamous Cell Carcinoma of the Larynx Image Gallery:
CASE NUMBER 155 Clinical History: A 62-year-old male died of bronchopneumonia. He was an alcoholic and ate poorly for many years. Gross: In the right lobe of the liver there was a circumscribed, dark red, spongy mass 4 cm in size. In the center of the mass there was a gray, firm, fibrous core. Microscopic: Naked eye inspection reveals a mass with many blood filled spaces. These are formed by anastomosing strands of connective tissue, partially hyalinized, lined by endothelial cells. Notice the subcapsular location of the tumor and its relationship to the liver parenchyma. DIAGNOSIS: Cavernous Hemangioma of Liver Image Gallery:
CASE NUMBER 158 Clinical History: A 63-year-old African American male had a five year history of progressive weakness and congestive heart failure. Gross: The left lung was dark red and heavy, and a large amount of hemorrhagic frothy fluid exuded freely from the cut surface. In the main pulmonary artery there was a large red firm clot adherent to the vascular wall. Many small blood clots were present in the vessels of the upper and lower lobes. Associated with these were many wedge-shaped, dark red, firmer areas in the lung parenchyma. Microscopic: There are two sections of most slides. On one slide there are organizing thrombi in the pulmonary arteries. On the other side there is a large hemorrhagic area in which some alveolar septa are pink, smudgy, and necrotic. In other portions of the lung the septa are thickened with fibrosis. DIAGNOSIS: Pulmonary Embolism and Hemorrhagic Infarct Image Gallery:
CASE NUMBER 159 Clinical history: This 45 year man complained of flushing, diarrhea, nausea and vomiting. Elevated levels of serotonin and its metabolite, 5-hydroxyindoleacetic acid, were found in the blood. An appendectomy was performed. Gross: The appendix is enlarged by a solid yellow tan tumor mass that protrudes into the lumen. Microscopic: The tumor cells are relatively small with a round to oval stippled nucleus. There is minimal variation in size and shape. By electron microscopy, the cells contain secretory granules. DIAGNOSIS: Carcinoid tumor of the appendix Image Gallery:
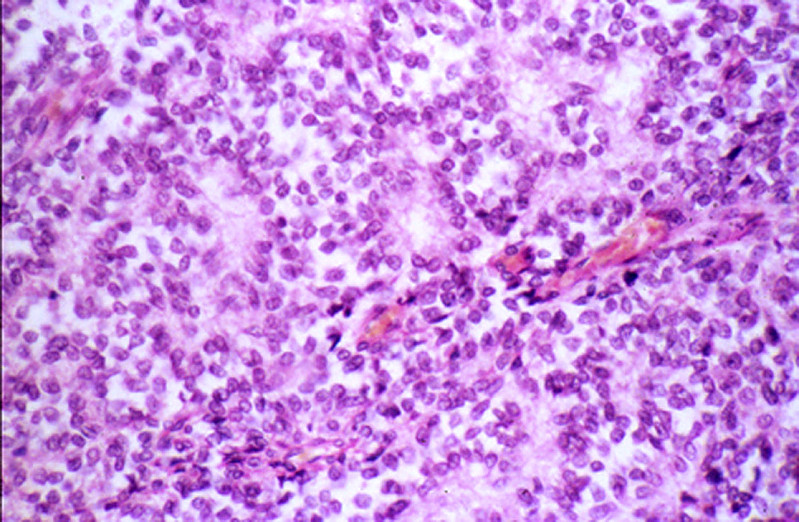
CASE NUMBER 161 Clinical History: This was a 16-year-old white male who complained a pain and swelling in his hip. He gave a history of having been struck by a baseball four months previously. Gross: The radiograph obtained at presentation shows soft tissue extension of the tumor. Cross section through the resected femoral head shows a soft tan white tumor with focal hemorrhage and necrosis. There is extensive soft tissue invasion. Microscopic: A striking feature is the monotony of the cells with round to oval vesicular nuclei and poorly defined, scanty eosinophilic cytoplasm. There are a moderate number of mitoses, but tumor giant cells and pleomorphism are conspicuously absent. The tumor cells are arranged around scanty, very vascular, fibrous stroma in a trabecular fashion, sometimes resembling rosette formation. In between these cords the tumor cells seem to line empty spaces. Histologically it is quite difficult to distinguish this tumor from a neuroblastoma. DIAGNOSIS: Ewing's sarcoma Image Gallery:
CASE NUMBER 166 Clinical History: A 43-year-old white female had a four-month history of intermittent bloody stools. Sigmoidoscopy revealed pedunculated polyps 15 cm above the sphincter. Gross: The resected tissue was a double stalked and double headed polyp of 1.5 cm in diameter. The stalk was 2 cm in length. The base of the stalk and the adjacent mucosa showed no induration. Microscopic: The exophytic structure of the polyp can be seen with the naked eye. There is a short stalk lined by normal colon mucosa with blood vessels in the submucosa. The finger-like villi of the polyp are lined by adenomatous mucosa, the hallmark of a neoplastic polyp. Compared to the nearby normal mucosa, the nuclei are elongated, hyperchromatic and stratified. There is increased nuclear to cytoplasmic ratio and decreased cytoplasmic mucin. DIAGNOSIS: Tubulovillous Adenoma (Polyp) of Colon Image Gallery:
CASE NUMBER 170 Clinical History: This was an incidental finding in the lung in a case of uremia due to chronic pyelonephritis in a 67-year-old white male. Gross: There was a hard, very well circumscribed, round nodule with a greyish glassy cut surface in the lung. Microscopic: There is normal cartilage, hyperplastic bronchial epithelium, and fragments of lung tissue with the alveoli filled with mononuclear cells derived from the alveolar epithelial cells. These lesions are common and seldom cause clinical symptoms. DIAGNOSIS: Cartilaginous Hamartoma Image Gallery:
CASE NUMBER 189 Clinical History: An 80-year-old white male had a three week history of chalky and greasy stools, a 20 pound weight loss, and a progressive obstructive jaundice. A cholangiogram revealed an obstruction in the common bile duct probably due to carcinoma of the pancreas. Gross: The head of the pancreas was enlarged with yellow-gray firm tissue, in which no normal lobular structures were seen. About 4 cm proximal to the ampulla there was a stenosis of the common bile duct. Proximal to this stenosis the bile ducts were markedly dilated with bile. The peripancreatic lymph nodes and the celiac axis were gray and firm with metastases of tumor. Microscopic: The tumor is composed of duct-like structures, which are irregularly arranged and infiltrate into the dense connective stroma and perivascular or perineural lymphatics. Occasionally both ducts and individual tumor cells contain mucin. There is a small amount of pancreatic tissue which shows marked atrophy and fibrosis. The small ducts are distended and may show focal squamous metaplasia of the epithelium in some sections. DIAGNOSIS: Adenocarcinoma of Pancreas Image Gallery:
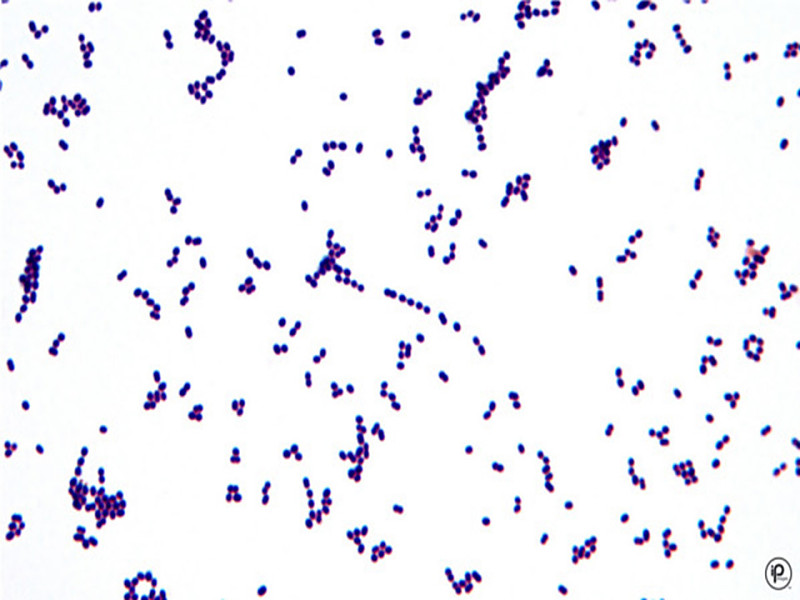
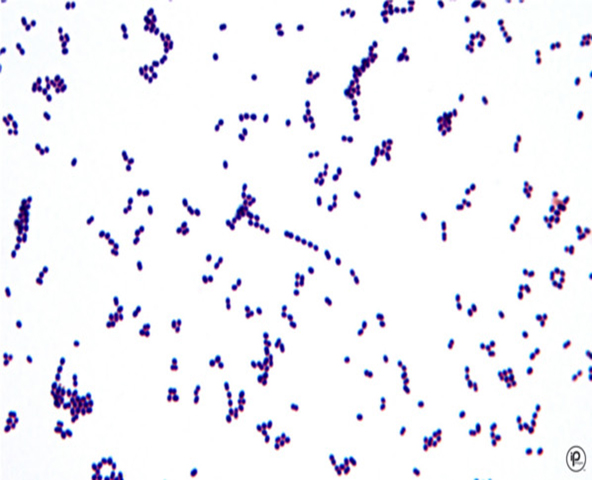
CASE NUMBER 195 Clinical History: A 67-year-old male had rheumatic heart disease for thirty years. Three months prior to death he began to have episodes of fever and chills accompanied by signs of worsening congestive heart failure. Splinter hemorrhages and purpuric skin rashes were noted three weeks before death. Lab Findings: Blood cultures grew alpha-hemolytic streptococci. Gram stain shows gram positive cocci in chains. Gross: The heart weighed 400 grams. There was thickening of the mitral valve leaflets and the chordae tendineae. Many friable calcified pink-gray granular verrucae were present on the valve. In addition, a large vegetation of the same type was found on the left auricular endocardium. Microscopis: The section represents a portion of mitral valve, left atrium and left ventricle. The valve is greatly thickened and damaged. It is infiltrated with acute and chronic inflammatory cells, and shows a zone of necrosis and fibrosis in the central portion of the valve. The myocardium shows slight focal fibrosis, and focal acute inflammatory infiltration in some sections. DIAGNOSIS: Infective (Bacterial) Endocarditis Image Gallery:
CASE NUMBER 199 (slide 033_ZZ) Clinical History: A 34-year-old woman discovered a mass in her breast. Gross: A 3 x 3 x 2 cm firm mass was found in the breast. Microscopic: Ductal carcinomas range from well-differentiated tumors characterized by good duct formation to poorly-differentiated tumors such as this one which is composed of sheets of pleomorphic cells which infiltrate into the adjacent breast tissue. This tumor also has evoked a strong lymphocytic response. A special form of breast cancer, referred to as medullary carcinoma, is also poorly-differentiated with an abundant lymphocytic response, but it is well-circumscribed and has a better prognosis than this tumor. Also note the adjacent normal breast lobules. In some there is also a lymphocytic infiltrate, though no tumor is seen in them. DIAGNOSIS: Infiltrating Ductal Carcinoma of the Breast Image Gallery:
CASE NUMBER 200 Clinical History: A 30-year-old white female noted intermittent pain and swelling of her knee for 1 1/2 years. She slipped on the stairs and suffered immediate severe pain in the knee. X-ray revealed a tumor which was a large area of decalcification with expansion of tibia, but with thinning of the cortex. The tumor was removed by curetting. Gross: The tumor tissue as illustrated from a different patient was a red-brown soft mass. Microscopic: The tumor is surrounded by a thin rim of cortical bone which is atrophic and shows focal periosteal bone formation. The tumor is composed of many large multinucleated cells and spindle cells resembling fibroblasts. Transitions between these two types of cells may be seen. Many dilated vessels are present in the tumor tissue. DIAGNOSIS: Giant cell bone tumor Image Gallery:
CASE NUMBER 202 Clinical History: A 74-year-old white man had hesitancy, intermittency, nocturia, and increasing difficulty in urination for one year. Rectal examination revealed an enlarged, nodular firm prostate. Gross: The prostate was large, nodular, and 120 grams in weight. The capsule was tense, and many gray-white firm nodules bulged out of the cut surface. These nodules varied from 3 mm to 1 cm. The larger ones were present in the lateral lobes and compressed the urethra. Microscopic: Two types of nodules can be distinguished. One is composed essentially of fibro-muscular elements - stromal hyperplasia. The other is composed predominantly of epithelial glands. The size of the glands varies remarkably, and cystic dilatation of some is present. There are two types of cells forming the glands. The lumenal cells are tall columnar cells with basal nuclei and apocrine secretory activity in the cytoplasm. The basal cell layer is composed of cuboidal or flattened epithelium. These glandular nodules are well demarcated by the encircling fibro-muscular stroma. DIAGNOSIS: Nodular Hyperplasia, Prostate Image Gallery:
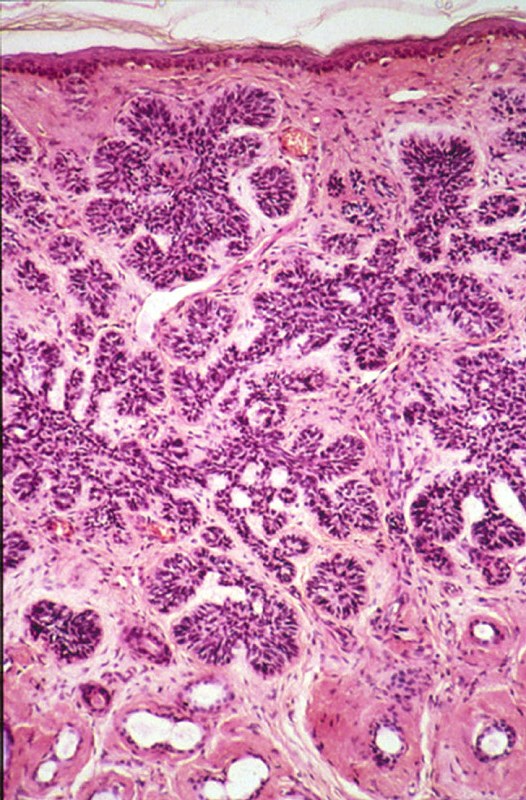
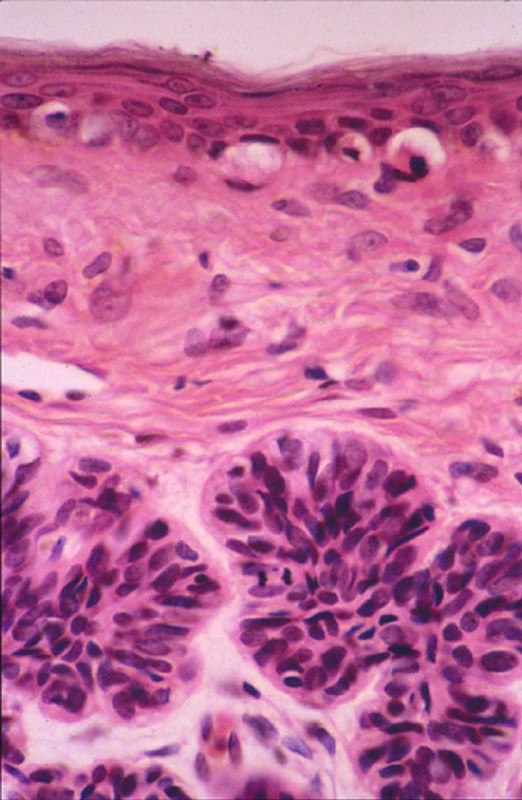
CASE NUMBER 203 Clinical History: 49-year-old man with a lesions on his hands. Gross: There is a 6 mm in diameter gray/tan lesion with a papillated surface. Microscopic: There is marked epidermal hyperplasia with a papillated surface, thickening of the granular layer (hypergranulosis) and cornified layer (hyperkeratosis). Within the granular layer, many of the cells contain large, coarse keratohyalin granules. There are foci of preservation of nuclei in the cornified layer (parakeratosis), especially overlying the tips of the papillae. The vessels in the papillary dermis are dilated. DIAGNOSIS: Verruca Vulgaris Image Gallery:
CASE NUMBER 220 Clinical History: This was a 58-year-old female whose uterus was removed along with the ovaries for an ovarian teratoma. Gross: The uterus was slightly enlarged, and contained many gray firm circumscribed nodules 0.5 cm - 2 cm in size. These nodules bulged out of the cut surface. Most of them were located intramurally, but there were some submucously and subserously located. Microscopic: The tumor nodules are composed of interlacing bundles of cells, which have long spindle nuclei and pink fibrillary cytoplasm. These cells resemble the smooth muscle cells of the myometrium. Portions of the tumor tissue have become pink hyalinized masses in which only a few cells are present. These tumor nodules do not have a definite capsule, though their outlines are rather distinct. A small number of vessels are present within the tumor. DIAGNOSIS: Leiomyoma of Uterus Image Gallery:
CASE NUMBER 223 Clinical History: A 13-year-old male had an enlarging mass in the left thigh for 1 1/2 months. It was not associated with pain or tenderness. The X-ray revealed a large tumor extending around the entire shaft and lower 1/3 or the left femur. Amputation was performed after biopsy. Gross: The tumor was a large, pink-gray, soft and granular mass, 8x4x5 cm in size, involving the lower femoral shaft, and growing into the muscle. Microscopic: The tumor is composed of sheaths of loosely packed fibroblastic and osteoblastic cells, which have large hyperchromatic nuclei and scanty eosinophilic cytoplasm. In the intercellular spaces of the tumor there is deposition of pink homogeneous osteoid tissue which frequently transforms into irregular, bony trabeculae. New periosteal bone formation may be seen in the section. DIAGNOSIS: Osteogenic Sarcoma of Bone Image Gallery:
CASE NUMBER 227 Clinical History: A 62-year-old white farmer entered with a complaint of a lesion on the right cheek of eight months duration. It had been growing slowly. Gross: There was a well circumscribed, firm, elevated mass 1 cm in diameter. The overlying skin was intact but smooth and somewhat dark colored. Microscopic: There are nests of darkly staining basophilic cells in the upper dermis with peripheral palisading. There is little cytoplasm, and the cytoplasmic borders are poorly defined. Nuclei are small and are round or oval, and occasional apoptotic bodies are noted. These tumors may arise from the basal cell layer of the epidermis or from dermal appendages. In this particular tumor there is an occasional round mass of keratin which is not usually seen in basal cell carcinomas. Note the loose, myxoid stroma about the tumor cells with some artifactual clefts. DIAGNOSIS: Basal Cell Carcinoma Image Gallery:
CASE NUMBER 229 Clinical History: This 6-month-old female experienced increased jaundice over a one month period. She died with pneumonia and liver failure. Gross: The liver was deep yellow and green after formalin fixation. The surface was nodular, and cut surfaces were firm. Microscopic: The liver architecture is completely replaced by fibrosis and regenerative nodule formation. In the broad fibrous bands separating regenerative nodules, there is abundant proliferation of bile ductules. The most striking feature of this liver is the severe cholestasis. Bile is seen in ducts, ductules and dilated cannuliculi. In scattered foci, it breaks into the liver parenchyma forming "bile lakes." DIAGNOSIS: Biliary liver cirrhosis Image Gallery:
CASE NUMBER 233 Clinical History: This 23-year-old white female was found to have a cervical lesion three months previous to this admission. A biopsy revealed carcinoma of the cervix. The uterus was removed. Preoperative radiation therapy is common today. Gross: The entire external cervix showed a large, gray-pink, fungating lesion, 5.5 cm in size. It extended into the internal cervical canal and also involved one of the obturator lymph nodes. Microscopic: The external cervix shows fibrosis and acute and chronic inflammatory infiltration. A portion of the cervical mucosa is infiltrated with squamous cell carcinoma. The tumor cells are pleomorphic and bizarre and frequently form giant cells. Strands and nests of the tumor cells are seen in the cervical stroma. Marked acute and chronic inflammation is present in association with the tumor. DIAGNOSIS: Squamous cell carcinoma of the cervix Image Gallery:
CASE NUMBER 240 Clinical History: This patient was a 54-year-old male who had a long history of peptic ulcer disease. In this instance both gastric and duodenal ulcers were found. Gross: The gastric mucosa was flattened in most areas, but demonstrated a focal thickening in the area of the ulcer, though no gross ulceration was detected. Microscopic: Microscopic sections show a portion of antral/pyloric stomach. A large ulcer and the accompanying response have replaced all layers of the stomach mucosa and wall. Three layers may be distinguished in the bed of the ulcer. The innermost one is composed of necrotic debris and fibrino-purulent exudate in which bacteria and yeast are present. The middle layer is a zone of granulation tissue made up of small vessels and acute and chronic inflammation. The deepest portion of the ulcer is made up of fibrous scar. Some of the arteries in the scar tissue may show sclerosis. The mucosa adjacent to the ulcer shows acute and chronic gastritis. Helicobacter pylori microorganisms can be discerned overlying the gastric mucosa in some sections. DIAGNOSIS: Chronic Gastric Ulcer Image Gallery:
CASE NUMBER 253 Clinical History: A 60-year-old female had a one year history of weight loss and upper gastro-intestinal obstruction for three months. Gross: The resected portion of the stomach showed a large fungating, partially ulcerated tumor mass in the antrum. Regional lymph nodes and a liver biopsy were free of tumor. Microscopic: There is a rather abrupt change of the normal stomach mucosa to malignant tumor tissue, projecting into the lumen as a cauliflower-like mass. The tumor forms abundant irregular acini, lined by one or more layers of atypical cells with mostly large irregular nuclei and poorly defined eosinophilic cytoplasm. Atypical mitoses are moderately frequent. The tumor has infiltrated through the muscularis mucosa and the edematous submucosa and has invaded the muscle layers. The invading tumor had elicited a rather marked neutrophilic and plasma cell response. DIAGNOSIS: Adenocarcinoma of Stomach (Intestinal Type) Image Gallery:
CASE NUMBER 264 Clinical History: A 38 -year-old white female complained of a mass in the neck of several months duration. At the time of examination the right lobe of the thyroid was enlarged and somewhat nodular. The opposite lobe was questionably enlarged. She had no symptoms of hypothyroidism or hyperthyroidism. Gross: At the time of surgery the entire thyroid was enlarged, with an estimated weight of 60 grams. The tissue was pale and lobulated. A subtotal thyroidectomy was performed. The excised tissue weighed 30 grams. Microscopic: The architecture of the gland is destroyed. A few acini are present. These vary in size. There is abundant lymphoid tissue in which are germinal centers. There are collections of rather large cells which do not form acini. DIAGNOSIS: Hashimoto's Thyroiditis Image Gallery:
CASE NUMBER 281 Clinical History: A 47-year-old female had an eight year history of refractory anemia and pancytopenia. She was treated with steroids. She was admitted shortly before death with fever and signs of infection. Gross: Multiple discrete nodules of the lung parenchyma along with thrombosed vessels were observed. Microscopic: The tissue reaction to the fungus infection cannot be seen well with this methenamine silver stain. It does bring out well the appearance of the Aspergillus with its septate hyphae and radial pattern of growth. DIAGNOSIS: Aspergillosis, Lung Image Gallery:
CASE NUMBER 286 Clinical History: This 64-year-old male had two episodes of myocardial infarction followed by congestive heart failure during the eight months prior to death. Death was preceded by arrhythmia. Gross: The heart was markedly hypertrophied (740 grams) and dilated. There was marked coronary atherosclerosis with an old occlusion of the left anterior descending vessel. A healed infarct involved the anteroseptal and apical region of the left ventricle. A mural thrombus covered much of the infarct within the heart cavity. Microscopic: The slide includes a transmural section of the anterior free wall and anterior portion of the interventricular septum. There is a broad band of dense, highly collagenized scar tissue replacing the middle layer of myocardium; patchy scarring interspersed with hypertrophied cardiac myocytes is present on either side of this dense scar. The endocardium is markedly thickened and there is organizing mural thrombus between cardiac trabeculae and extending into the lumen. Some myocytes in the subendocardial layer show sarcoplasmic vacuolization, a chronic degenerative change termed "myocytolysis". DIAGNOSIS: Healed myocardial infarct Image Gallery:
CASE NUMBER 294 History: The patient is a healthy 65-year-old male who was noted to have slightly
enlarged axillary and cervical lymph nodes on an annual physical examination. The
patient offered no complaints and was given a "clean bill of health" one year
previously. No organomegaly was noted. The CBC showed: WBC = 45,000 cells/mm3,
Hb = 13.5 gm/d., platelets = 185,000/mm3. Microscopic: Too many small, resting lymphocytes with soccer-ball nuclei (absolute lymphocytosis). Otherwise unremarkable. DIAGNOSIS: Chronic lymphocytic leukemia (B-cell)
CASE NUMBER 295 Clinical History: A 16-year-old boy presented with cervical lymphadenopathy and was found to have a mediastinal mass. The neck node was biopsied. Gross: The lymph node was enlarged, and remarkable for fibrous bands separating areas of firm, fleshy material. Microscopic: The normal lymph node architecture is completely destroyed. In its place are thick bands of collagen, separating islands of lymphoid tissue. In some of these nodules, there is a mixed infiltrate consisting of lymphocytes, eosinophils, some neutrophils and plasma cells, and numerous large cells with highly pleomorphic nuclei. Nuclei are frequently multi lobulated but classic binucleate Reed-Stemberg cells are uncommon. Many cells are so-called "lacunar variants", with nuclei which have artefactually shrunken away from their cytoplasmic borders, leaving a clear space than can often easily be appreciated at low power. DIAGNOSIS: Hodgkin's lymphoma, nodular sclerosing Image Gallery:
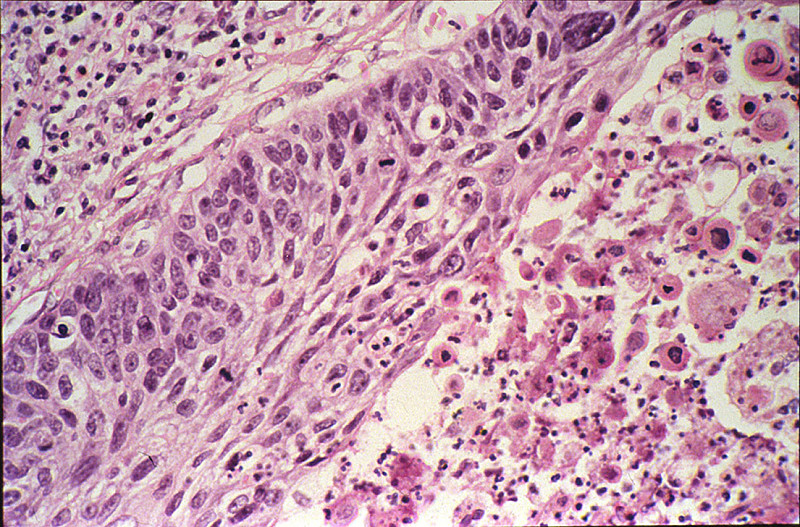
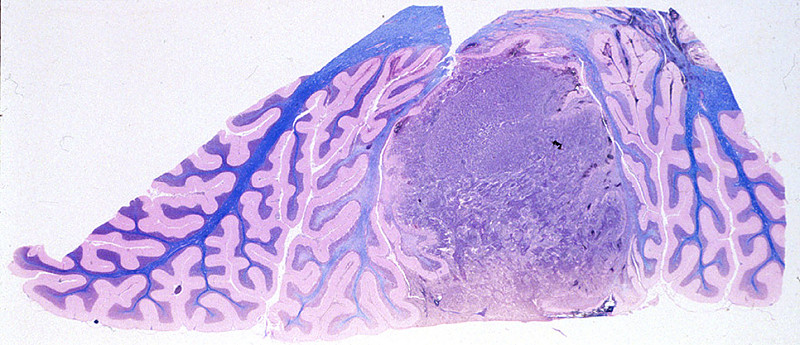
CASE NUMBER 329 Clinical History: This 16-year-old female had a four month history of headache. She developed seizures one week prior to death and was found to have a coarse vertical nystagmus and papilledema. At surgery, a posterior fossa tumor was found. Gross: A medulloblastoma was found in the anterior mid-cerebellum and extending laterally into the right lobe. It measured 2xIx1 cm. There was some tumor infiltration into the dentate nucleus. Microscopic: The section shows cerebellum with a pink molecular layer. Underlying that is the Purkinje cell layer composed of lage pyramidal neurons. Next is the granular cell layer. Granule cells are neurons. They are the cell on origin of medulloblastoma. Not the similar appearance to the tumor cells. The tumor consists of cells with round or oval dark staining nuceli. Mitotic figures are present. The white matter of the cerebellum stains blue with the luxol fast blue stain. (Luxol Fast Blue - H&E stain) DIAGNOSIS: Medulloblastoma Image Gallery:
CASE NUMBER 370 Clinical History: The patient was a 67-year-old white female who became disoriented and confused ten days prior to death and developed clumsiness on the left side of the body. She had vertigo (sensation of the room spinning) and a leftward-beating nystagmus (eyes drifting slowly to her right and then quickly darting back to her left). Her left eyelid drooped (ptosis) and her left pupil was constricted (miosis). A sensory exam showed loss of pain sensation on the right side of her body (limbs and trunk) and the left side of her face. Gross: There was thrombosis of the posterior inferior cerebellar artery (PICA). There was extensive necrosis of the left posterior, inferior cerebellum and left lateral anterior medulla. Microscopic: There is an area of liquefactive necrosis in which many macrophages with phagocytosed fat and myelin particles are present. Around this area are numerous large astrocytes with large vesicular nuclei and abundant eosinophilic cytoplasm. The myelin in this area stains very pale due to surrounding edema fluid. The blood vessels are congested and there is some extravasated blood. (Luxol Fast Blue - H&E stain) DIAGNOSIS: Infarct of Cerebellum and lateral medulla Image Gallery:
CASE NUMBER 371 Clinical History: The patient was a 67-year-old white female who became disoriented and confused ten days prior to death and developed a weakness on the left side of the body. She had difficulty with vision in the right eye and the retinal artery pressure was decreased on the right. Gross: There was thrombosis of the right internal carotid artery just above the bifurcation. There was extensive necrosis of the right frontal, parietal and temporal lobes and basal ganglia. Microscopic: There is an area of liquefactive necrosis in which many macrophages with phagocytosed fat and myelin particles are present. Around this area are numerous large astrocytes with large vesicular nuclei and abundant eosinophilic cytoplasm. The myelin in this area stains very pale due to surrounding edema fluid. The blood vessels are congested and there is some extravasated blood. DIAGNOSIS: Cerebral Infarction Image Gallery:
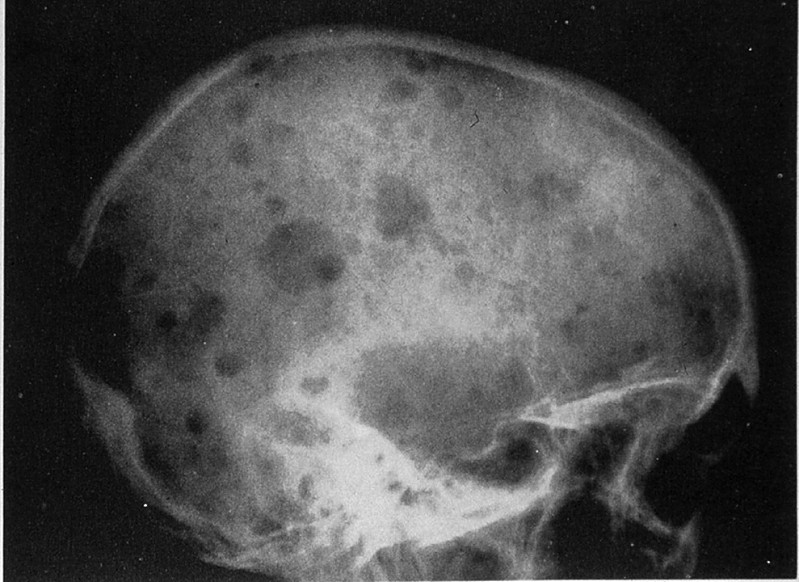
CASE NUMBER 413 Gross: Many of the bones contained poorly delineated, soft gelatinous red tumor masses of various dimensions. Plain film of the skull shows sharply punched out bone lesions. Microscopic: The marrow is heavily infiltrated with plasma cells which vary in degree of maturation. Islets of normoblasts are present, but granulocytes and megakaryocytes are markedly decreased. There is considerable loss of trabecular and cortical bone. DIAGNOSIS: Multiple myeloma Image Gallery:
CASE NUMBER 427 Clinical History: A 78-year-old male was admitted with headache and bitemporal hemianopsia of several years duration. No endocrine disturbances were noted. Gross: The pituitary gland, weighing 3gms and measuring 2 cms in greatest diameter, contained a large pink-gray soft tumor mass in the anterior lobe. The optic chiasm was slightly atrophic due to the compression of the tumor. Microscopic: The tumor occupies nearly the entire anterior lobe, so that only a thin rim of normal hypophyseal tissue is present in the subcapsular area. The tumor is composed of uniform cells arranged in a trabecular or sinusoidal pattern. The stroma is highly vascular. Some of the tumor cells contain fine eosinophilic granules, but most of them are chromophobes with special stains. DIAGNOSIS: Chromophobe Adenoma, Pituitary Image Gallery:
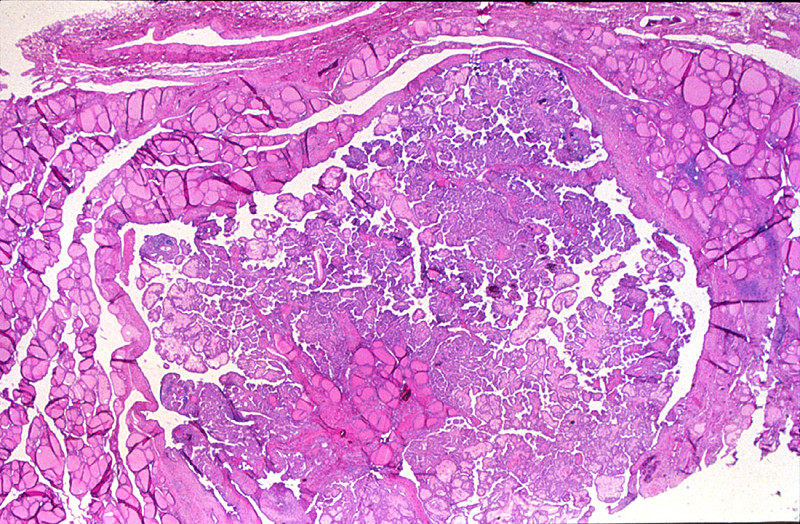
CASE NUMBER 429 Clinical History: A 50-year-old female had a slowly growing mass in the anterior cervical area for two years. Recent to her admission she had obstruction symptoms and hoarseness. No thyrotoxic manifestations were noted. A subtotal thyroidectomy was performed. Gross: The thyroid was nodular and weighed 250 grams. The capsule was intact. The cut surface revealed large and small honeycombed structures filled with yellow-brown colloid material. Focal hemorrhages and fibrosis were present in the nodules. Microscopic: The nodules consist of small and large follicles up to 3 mm in diameter. The epithelium is low cuboidal, and the colloid is rich. In some sections there is scalloping at the periphery of the colloid. There is fibrosis as well as focal recent and old hemorrhages. A small amount of atrophic, compressed thyroid tissue, may be seen in some sections. DIAGNOSIS: Colloid Nodules of Thyroid (Hyperplastic Thyroid) Image Gallery:
CASE NUMBER 430 Clinical History: A 23-year-old man presented with a nodule in his neck. Gross: The patient was found to have an enlarged lymph node and a thyroid nodule. Microscopic: The lesions in the lymph node and thyroid are similar. The tumor is composed of papillae covered by closely packed cells with bland, sometimes optically-clear ("Orphan-Annie eye") nuclei. Nuclear grooves are also present. A few round purplish calcifications, termed psammoma bodies, are also seen. DIAGNOSIS: Papillary Carcinoma of the Thyroid Image Gallery:
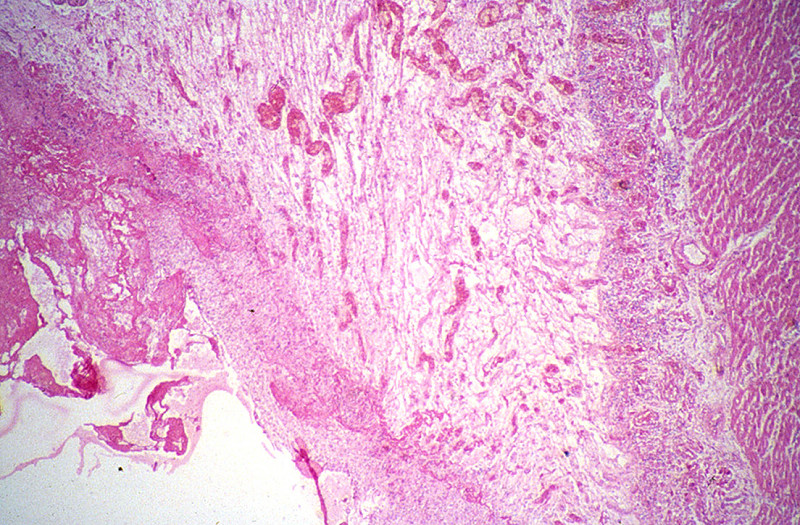
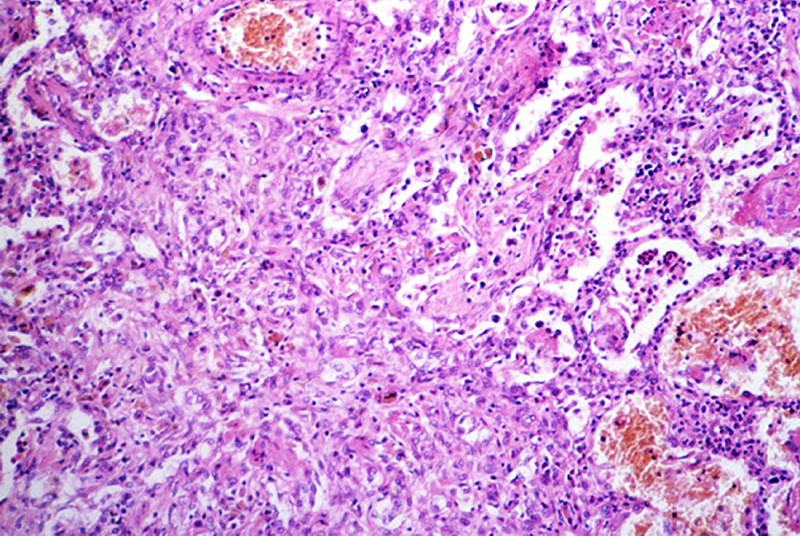
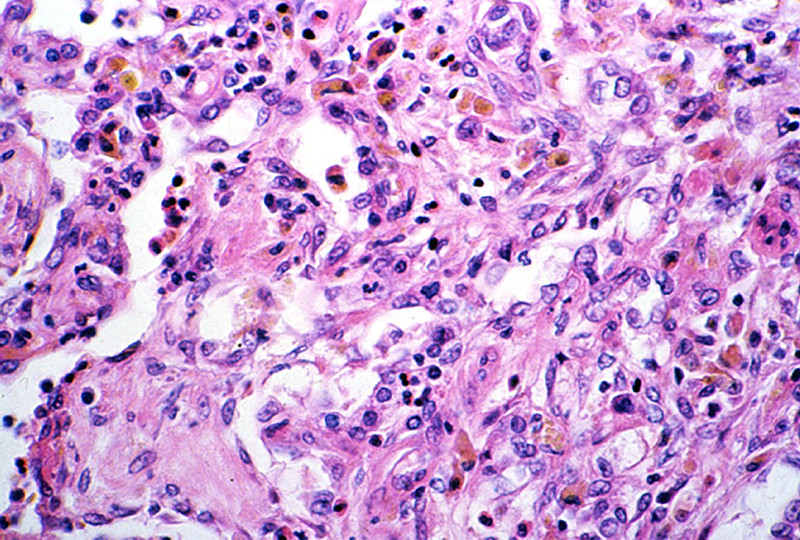
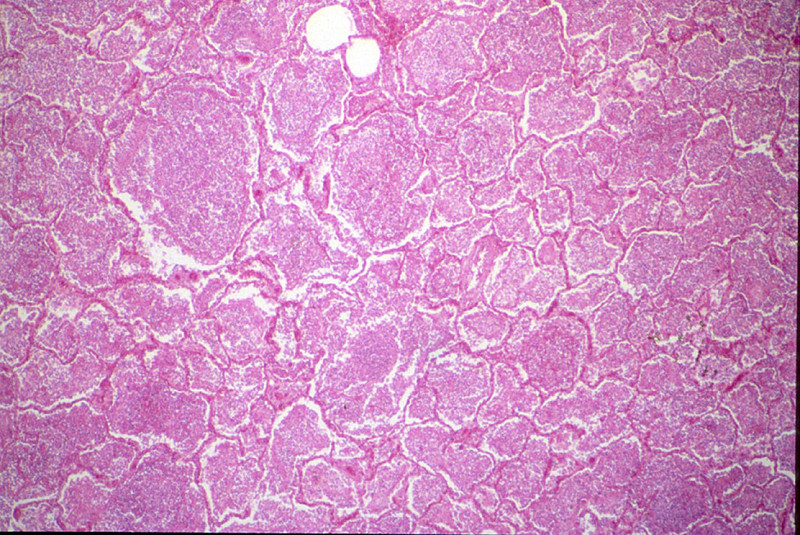
CASE NUMBER 451 Clinical History: A 4-year-old female had a gradual onset of fever, productive cough, anorexia and diarrhea about eleven days prior to death. The breathing sounds were harsh, and a few cracking rales were heard over the right base posteriorly. Gross: The lungs showed fibrinous exudates over the pleural surfaces. The cut surface of the lung revealed innumerable small, gray-white nodules 1-4 mm in size. A large caseous tubercle of 0.5 cm was present in the left lower lobe, eroding into a large pulmonary vessel. Microscopic: A lower power examination reveals numerous poorly defined tubercles approximately of the same size and same stage of development. These tubercles show a slight caseous necrosis and consist predominantly of mononuclear cells, epitheloid cells, and a few giant cells. In alveoli there is a moderate amount of mononuclear cell infiltration. Some lymphocyte and plasma cell infiltration is diffusely present in the alveolar septa. DIAGNOSIS: Miliary Tuberculosis of Lung Image Gallery:
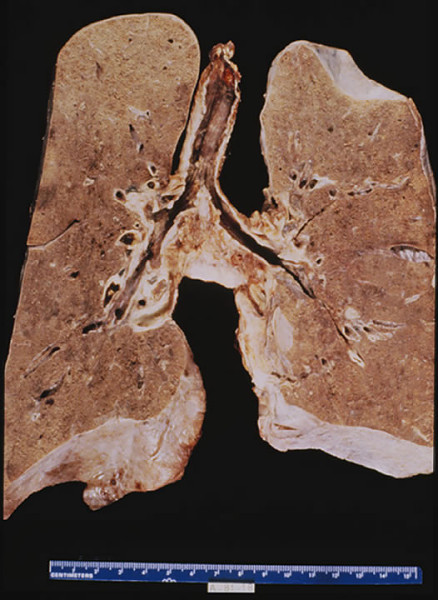
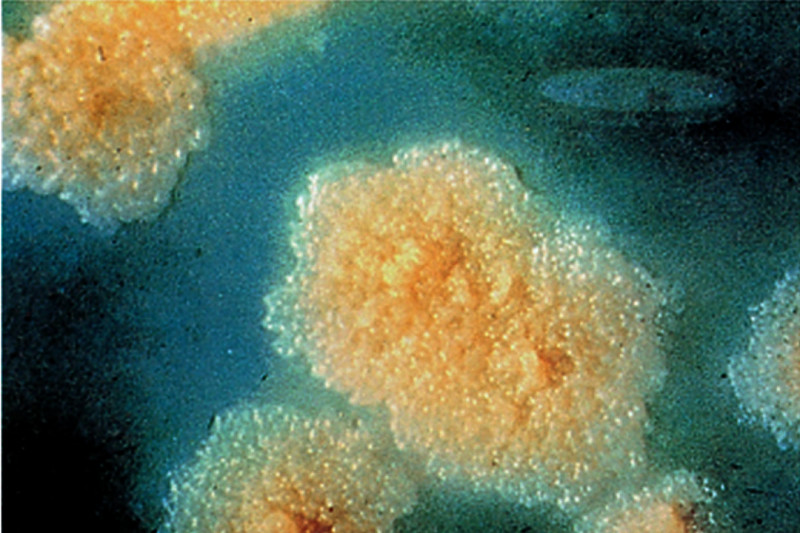
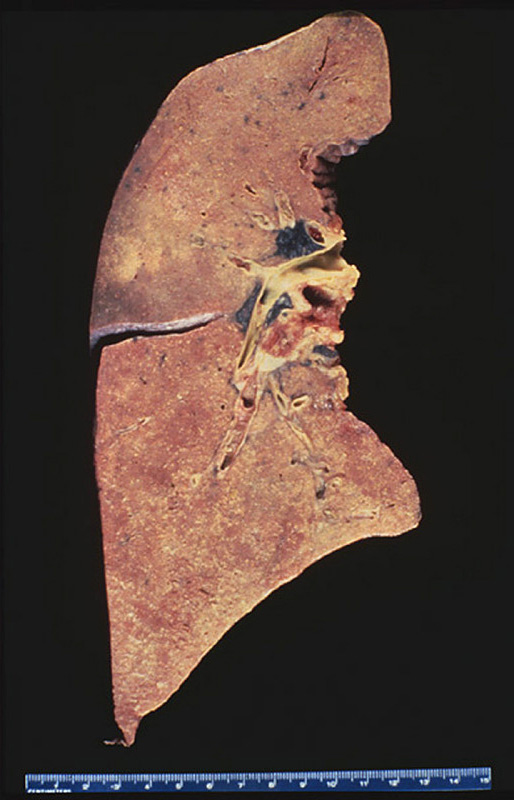
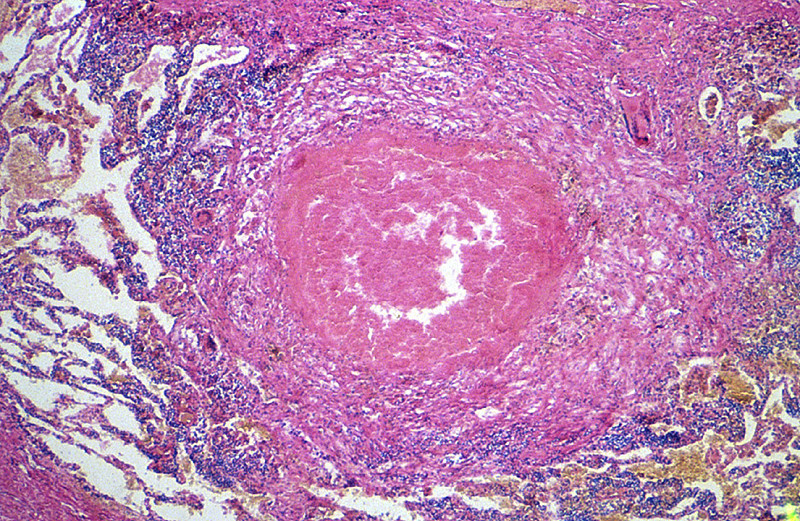
CASE NUMBER 452 Clinical History: A 50-year-old African American female had chronic cough, chest pain, night sweats and a swollen abdomen for the past four years. Gross: The lungs were heavy and had fibrous pleural adhesions. A large cavity containing caseous material was found in the apex of the left lung. The cavity communicated with a bronchus. In the left lower lobe there was large area of consolidation, which exuded creamy, yellow-gray, caseous material from the cut surface. Microscopic: This section shows many foci of caseous necrosis, which is associated with marked proliferation of histiocytes around the caseous foci. A small bronchus (not present in all sections) shows squamous metaplasia. DIAGNOSIS: Caseous Pulmonary Tuberculosis Image Gallery:
|
||